Home / Blog
Axipro Resource Hub
Latest Articles

Most organizations think their AI governance is further along than it is. McKinsey’s 2026 AI Trust Maturity Survey of roughly 500 organizations found an average maturity score of 2.3 out of 4, and only about a third reported level three or higher in strategy, governance, and agentic AI oversight. Adoption is outpacing control, and regulators have noticed. An AI governance maturity model gives you a way to measure that gap honestly. This guide covers what a maturity model is, the six dimensions it should measure, the five levels most models use, and how to assess your own organization and build a roadmap to the next level. What Is an AI Governance Maturity Model? An AI governance maturity model is a structured framework that describes how capable an organization is at governing its AI systems, usually across five progressive levels. The concept borrows directly from the Capability Maturity Model (CMM) that software engineering has used since the early 1990s: define the capability, describe what it looks like at each stage of development, and score yourself against it. The purpose is diagnosis. A maturity model tells you where governance is strong, where it’s theater, and where it doesn’t exist at all. How It Differs from General AI Governance Frameworks Frameworks like the NIST AI Risk Management Framework or ISO/IEC 42001 tell you what good governance contains: policies, risk assessments, accountability structures, monitoring. A maturity model tells you how well you’re doing those things today. The framework is the destination. The maturity model is the odometer. That distinction matters in practice. Plenty of companies can point to an AI policy document. Far fewer can show that the policy changes what teams actually ship. Why Enterprises Need a Maturity Model Three reasons. First, budget: you can’t prioritize governance investment without knowing which dimension lags. Second, accountability: a maturity score gives boards something concrete to track quarter over quarter. Third, regulation: the EU AI Act and frameworks like ISO 42001 assume a functioning management system, and a maturity assessment is the fastest way to find out whether yours would survive scrutiny. Core Dimensions of an AI Governance Maturity Model A useful model measures more than policy coverage. Six dimensions show up consistently across the credible models, including the IEEE-USA flexible maturity model built on the NIST AI RMF. Strategy and leadership. Does the organization have a stated position on AI risk, an executive owner (increasingly a Chief AI Officer), and board visibility? Gartner’s 2025 polling found 55% of organizations now have an AI board or dedicated oversight committee, which means nearly half still govern by improvisation. Policies, standards, and accountability. Written policies mapped to regulations, a RACI matrix for AI decisions, and clear escalation paths. Many organizations adapt the three lines of defense model from financial risk: the teams building AI, the risk function overseeing them, and internal audit checking both. Data governance and model lifecycle. Training data lineage, quality controls, and lifecycle management from development through deployment, monitoring, and retirement. This is where AI governance meets MLOps, and where mature organizations maintain an AI register, a live inventory of every model and system in production. Risk, compliance, and ethics. Risk classification of AI systems, impact assessments, bias and fairness testing, and explainability requirements. Banks will recognize the DNA of model risk management under SR 11-7 here. People, skills, and culture. Training, role clarity, and whether people outside the governance team actually understand their obligations. Tools, automation, and monitoring. Drift detection, automated policy checks, audit logging, and dashboards. Governance that lives in spreadsheets caps out around level three. The 5 Levels of AI Governance Maturity Level 1: Ad Hoc / Initial AI use happens without oversight. There’s no inventory, no policy, or a policy nobody follows. Shadow AI is common, and risk surfaces only when something breaks publicly. Level 2: Developing / Repeatable Someone has been assigned responsibility. A draft policy exists, a partial inventory exists, and reviews happen for high-profile projects. The practices are repeatable but depend on specific people rather than defined processes. Level 3: Defined / Structured Governance is documented, standardized, and applied across the organization. There’s a governance committee, a risk classification scheme, defined lifecycle gates, and mandatory training. Most organizations pursuing ISO 42001 certification are working to reach and formalize this level. Level 4: Managed / Metrics-Driven Governance produces numbers. Coverage rates, review cycle times, incident counts, and risk reduction are measured and reported to leadership. Controls are enforced by tooling rather than goodwill, and audits confirm the system works as described. Level 5: Optimized / Adaptive Governance improves itself. Monitoring feeds back into policy, controls adapt to new model types (agentic systems being the current test), and the organization anticipates regulatory change rather than reacting to it. Almost nobody is here yet, and that’s fine. Level 5 is a direction, not a deadline. Insider Note: In assessments, the most common self-scoring error is claiming level 3 on the strength of documents alone. If your policy says every model gets a pre-deployment review and your inventory shows 40 models but your review log shows 6, you’re at level 2. Evidence beats paperwork every time, and auditors check the logs first. AI Governance Maturity Matrix The matrix crosses dimensions with levels so you can score each one independently. Organizations are rarely uniform: it’s normal to sit at level 3 on policy and level 1 on monitoring. For scoring, keep the rubric simple: 1 to 5 per dimension, scored on evidence you could show an auditor, not on intentions. Board-level indicators (does the board see AI risk reporting?) and operational indicators (does every production model have a completed impact assessment?) should be scored separately, because they fail independently. How to Assess Your Current AI Governance Maturity Start with a baseline self-assessment. Pull together a cross-functional group covering engineering, legal, risk, security, and the business owners of major AI use cases, and score each dimension against the matrix. Half a day is usually enough for a first pass. For each dimension, the

Most organizations get ISO 42001 certified in 2 to 9 months. Companies that already hold ISO 27001 regularly land in the 2 to 5 month range, while enterprises with sprawling AI portfolios and no existing management system can take 12 months or more. The audit itself only takes days. Almost the entire calendar goes into building and operating your AI Management System (AIMS) long enough to produce evidence an auditor can actually check. That is the short answer. The longer answer depends on your starting point, your scope, and how quickly you can get a certification body on the schedule. This article breaks down the full timeline phase by phase, the factors that stretch or compress it, and what the recertification cycle looks like once you hold the certificate. Typical ISO 42001 Certification Timeline at a Glance ISO/IEC 42001:2023 is the first international standard for AI management systems, published in December 2023. Because it follows the same harmonized structure as ISO 27001 and ISO 9001, the certification process will feel familiar to anyone who has been through a management system audit: build the system, run it, pass a Stage 1 and Stage 2 audit, then maintain it through annual surveillance. Here is how timelines typically break down by company size. Average Timeline for Small Businesses Small companies move fastest because scope stays contained. A startup with two or three AI systems, a handful of decision makers, and short approval chains can finish scoping in a week and get policies signed off in days rather than weeks. The realistic floor for a small business starting from scratch is around 3 months. With an existing ISO 27001 program and a compliance platform already collecting evidence, 2 months is achievable. Average Timeline for Mid-Sized Companies Mid-sized companies usually take 6 to 9 months. The AI inventory is growing, more departments are touching AI systems, and risk assessments have to cover more use cases. Coordination becomes the hidden cost: getting engineering, legal, and product to agree on an AI policy takes longer than writing the policy itself. Average Timeline for Enterprises Enterprises should plan for 9 to 12 months, sometimes longer. The main drivers are AI system sprawl across business units, longer procurement cycles for certification bodies, and audits that take more days. The Stage 2 audit for a large multinational can run two weeks or more on its own, and internal alignment before the audit takes far longer than the audit itself. Breakdown of the ISO 42001 Certification Timeline by Phase The phases below overlap in practice. Treat the durations as effort estimates for a reasonably resourced program, not a strict sequence. Phase 1: Scoping and Gap Analysis (2–4 Weeks) Everything starts with two questions: which AI systems are in scope, and how far is your current governance from what the standard requires? The gap analysis maps your existing policies and controls against the standard’s clauses and Annex A controls, and produces the project plan for everything that follows. Get the scope wrong here and every later phase inherits the mistake. Phase 2: AIMS Design, Leadership, and AI Policy Development (2–4 Weeks) This phase establishes the skeleton of the management system: the AI policy, governance roles, objectives, and the leadership commitments the standard requires. Executive sign-off is the gating item. The documents are not hard to write. Getting senior leadership to formally own AI governance is where programs stall. Phase 3: AI Risk and Impact Assessments (2–6 Weeks) ISO 42001 requires both AI risk assessments and AI impact assessments, and the distinction matters. Risk assessments look at what could go wrong for the organization. Impact assessments look at consequences for individuals and society, which is a newer discipline for most teams. This phase takes longer when you have many AI systems, high-risk use cases, or no prior methodology to adapt. The output feeds directly into your Statement of Applicability (SoA), the document that maps which Annex A controls you have selected and why. Insider Note: Impact assessments are where auditors probe hardest, because they are the most distinctive part of ISO 42001 compared with ISO 27001. A recycled security risk register with “AI” pasted into it will get picked apart in Stage 2. Build the impact assessment methodology properly the first time. Phase 4: Controls Implementation (2–10 Weeks) The longest phase. Here you implement the Annex A controls selected in your SoA: AI system lifecycle documentation, data governance for training data, human oversight mechanisms, transparency measures, supplier management for third-party AI, and so on. Duration depends almost entirely on the gap analysis results. Organizations with mature engineering practices often find they already do much of this and just need to document it. Organizations without formal AI development processes are building from zero. Phase 5: Documentation, Training, and Evidence Collection (2–8 Weeks) Certification requires proof that the system operates, not just that it exists on paper. That means records: training completion logs, risk assessment outputs, review meeting minutes, monitoring reports. This phase runs partly in parallel with implementation, but it cannot be compressed below a certain floor because auditors want to see evidence generated over time, not a folder of documents all created the week before Stage 1. Phase 6: Internal Audit and Management Review (2–4 Weeks) The standard requires an internal audit of the AIMS and a formal management review before the certification audit. This is your dress rehearsal. A good internal audit surfaces nonconformities while they are still cheap to fix. Skipping or rushing it is a false economy that shows up later as Stage 2 findings. Phase 7: Stage 1 Certification Audit (1–2 Weeks) The certification body reviews your documentation and assesses readiness for Stage 2. The audit itself takes 1 to 3 days for most organizations. The auditor examines your scope statement, AI policy, risk and impact assessment methodology, SoA, and internal audit results, then issues findings. The 1–2 week window covers the audit plus the report. Phase 8: Closing Nonconformities (2–4 Weeks) Almost every Stage 1 produces findings.

CMMC requirements started appearing in Department of Defense contracts on November 10, 2025, when the final DFARS rule took effect. By November 10, 2028, the clause at DFARS 252.204-7021 must appear in every solicitation and contract where contractor systems process, store, or transmit Controlled Unclassified Information (CUI). For most of the Defense Industrial Base (DIB), the math is blunt: pass a CMMC assessment or lose eligibility for DoD work. A CMMC readiness assessment is how you find out whether you’d pass before the stakes are real. It’s a structured review of your environment, documentation, and evidence against the requirements of the Cybersecurity Maturity Model Certification, done before you sit for a self-assessment or a Certified Third-Party Assessment Organization (C3PAO) audit. A good one tells you exactly where you stand and what to fix first. This guide covers what a readiness assessment includes, how the process works at each CMMC level, what it costs, how long it takes, and how to pick someone to run one. What Is a CMMC Readiness Assessment? A CMMC readiness assessment is a pre-certification evaluation that measures your organization against the specific requirements of your target CMMC level. It examines your scope, implemented controls, System Security Plan (SSP), Plan of Action and Milestones (POA&M), and the evidence supporting them, then produces a gap analysis and a remediation roadmap. The purpose is simple: surface every deficiency while it’s still cheap to fix. An assessor who finds a scoping error during a readiness review costs you a few weeks of rework. A C3PAO who finds the same error during a certification assessment can cost you the assessment fee, months of delay, and in some cases contract eligibility. How It Differs From an Official C3PAO Audit An official CMMC Level 2 certification assessment is conducted by a C3PAO accredited by the Cyber AB, the official accreditation body for the CMMC ecosystem. The C3PAO’s findings are binding. Results go into the DoD’s assessment systems, and a passing result produces a CMMC status that contracting officers verify before award. A readiness assessment carries no official weight. Nothing gets filed or certified, and a poor result costs you nothing beyond the work needed to fix it. That’s the whole point. It’s the only stage in the entire process where failure is free. There’s also a conflict-of-interest rule worth knowing. A C3PAO cannot provide consulting and remediation services to an organization and then certify that same organization. If a C3PAO helps you prepare, a different C3PAO has to assess you. How It Differs From a Mock Assessment A mock assessment is a dress rehearsal. It simulates the certification assessment itself: assessors interview control owners, request evidence on the spot, and score findings the way a C3PAO would. A readiness assessment is broader and comes earlier, and its job is discovering and closing gaps rather than rehearsing the exam. Most organizations run a readiness assessment first, remediate, then run a mock assessment a few weeks before the real one to see whether staff and evidence hold up under live questioning. How It Differs From a Self-Assessment A self-assessment is a formal CMMC mechanism rather than a preparation exercise. CMMC Level 1 and a subset of Level 2 contracts let organizations self-assess, post the results to the Supplier Performance Risk System (SPRS), and have a senior official affirm compliance annually. That affirmation is a representation to the government, and false or careless affirmations carry False Claims Act exposure. A readiness assessment is the check you run before making that representation, so the number you affirm reflects reality. Why a CMMC Readiness Assessment Matters Avoiding Failed Certification Attempts CMMC Level 2 covers all 110 security controls of NIST SP 800-171, evaluated against 320 assessment objectives. Every objective has to be met for a control to score, and there’s no partial credit. Organizations that skip readiness work routinely walk into certification believing they’re compliant because controls are “mostly” implemented. Mostly implemented scores the same as not implemented. Protecting DoD Contract Eligibility Under the phased rollout that began in November 2025, CMMC status is a condition of award. Prime contractors also have to flow the requirement down to subcontractors that handle Federal Contract Information (FCI) or CUI, and they’ve been pushing their supply chains hard. So a missed certification hurts twice: you lose the immediate contract, and you risk dropping out of a prime’s approved supplier pool during the exact window when those pools are being rebuilt around CMMC status. Reducing Remediation Costs and Delays Gaps found early get fixed on your schedule with your choice of solution. Gaps found during certification get fixed under deadline pressure, often with whatever expensive tooling can be deployed fastest. There’s a conditional CMMC status for organizations that pass with a limited POA&M, but closeout has to happen within 180 days, and only certain lower-weighted controls are POA&M-eligible in the first place. Readiness work keeps you out of that corner. Worth Knowing: The DoD Assessment Methodology The DoD Assessment Methodology weights each NIST SP 800-171 control at 1, 3, or 5 points, deducted from a starting score of 110. The floor is -203. To achieve even a conditional Level 2 status, you need a minimum score of 88. A handful of unmet 5-point controls, such as FIPS-validated encryption or multifactor authentication, can put certification out of reach on their own, so a readiness assessment should always show the point weight attached to every gap. When to Conduct a CMMC Readiness Assessment Before your first self-assessment. If a contract requires a Level 1 or Level 2 self-assessment, run readiness work before you post a score to SPRS. The score you affirm is a legal representation, and it’s far easier to fix the environment than to explain a misstated score later. When contract requirements are approaching. If CMMC language has shown up in a solicitation you plan to bid, or your prime has set a certification deadline, count backward. Remediation after a readiness assessment typically takes six to twelve months for organizations starting

CMMC certification costs between $4,000 and $30,000 at Level 1, $30,000 to $300,000 or more at Level 2, and $100,000 to well over $1 million at Level 3. Most contractors expect the audit fee to be the big number. It isn’t. The formal assessment typically accounts for only 25% to 40% of total spend, with preparation, remediation, and technology upgrades consuming the rest. The stakes changed in late 2025. The final 48 CFR acquisition rule took effect on November 10, 2025, which means CMMC requirements now appear directly in Department of Defense (DoD) solicitations and contracts. Starting in November 2026, Phase 2 of the rollout gives contracting officers the authority to require third-party certification for Level 2 work. If you handle Controlled Unclassified Information (CUI), certification is no longer optional, and the cost question becomes a budgeting exercise rather than a hypothetical. This guide breaks down every major cost category, what moves your number up or down, and how to keep the total under control. What Is CMMC Certification and Why Does Cost Vary? The Cybersecurity Maturity Model Certification (CMMC) is the DoD’s framework for verifying that companies in the Defense Industrial Base (DIB) actually protect the sensitive information they handle. The program, codified in 32 CFR Part 170, builds on the security requirements of NIST SP 800-171 and, at the top tier, selected controls from NIST SP 800-172. Costs vary so widely because you can’t buy CMMC off a shelf. Your environment has to reach a certain state and then stay there. A 15-person machine shop with one well-scoped CUI enclave faces a fundamentally different project than a 500-person prime contractor with CUI flowing through a dozen systems. Your starting security posture, the scope of your assessment boundary, and whether you build internally or hire help all move the total by six figures in either direction. Average CMMC Certification Cost at a Glance The DoD’s own published estimates are instructive. A triennial Level 2 certification assessment, including affirmations, is projected at roughly $105,000 for small entities and $118,000 for larger ones. Those figures cover only assessment and affirmation activities, though. The DoD excludes implementation costs from its estimates on the grounds that NIST SP 800-171 compliance has been contractually required under DFARS 252.204-7012 since 2017. Your real budget has to cover both. CMMC Certification Cost by Level CMMC Level 1 (Foundational) Cost: $5,000 – $30,000 Level 1 covers Federal Contract Information (FCI) and requires 15 basic safeguarding practices drawn from FAR 52.204-21. Because Level 1 permits an annual self-assessment with no third-party auditor, the costs are internal labor, basic tooling, and documentation. Small contractors with reasonable IT hygiene often land near the bottom of the range. The DoD estimates annual Level 1 assessment and affirmation activity at around $6,000 for a small entity, with the remainder of the range driven by any remediation needed to attest honestly. CMMC Level 2 (Advanced) Cost: $50,000 – $300,000+ Level 2 is where most of the DIB lands and where budgets get serious. It requires full implementation of all 110 security requirements in NIST SP 800-171, assessed across 320 individual objectives. For most contracts, a C3PAO (Certified Third-Party Assessor Organization) accredited by the Cyber AB has to conduct the assessment every three years. Market data puts C3PAO assessment fees at $30,000 to $100,000 depending on scope, site count, and complexity. Preparation dwarfs that figure for most organizations. Companies starting from a low maturity baseline routinely spend three to four times the assessment fee on readiness work before an auditor ever shows up. CMMC Level 3 (Expert) Cost: $300,000 – $1,000,000+ Level 3 adds 24 enhanced requirements from NIST SP 800-172 on top of a completed Level 2 certification, and the assessment is conducted by the government’s DIBCAC rather than a commercial C3PAO. DIBCAC charges no assessment fee, but don’t mistake free for cheap. The DoD estimated roughly $41,000 in additional implementation cost for the 800-172 controls alone, and total triennial assessment-related costs in the $146,000 to $159,000 range. Real-world totals run far higher once you account for the advanced tooling, threat hunting capability, and organizational changes Level 3 demands. Only contractors supporting the most sensitive programs need this tier. Worth Knowing: You can’t skip to Level 3. You can’t skip to Level 3. A final Level 2 certification with all POA&M items closed is a prerequisite for the same assessment scope, so Level 3 budgets always include a full Level 2 project first. CMMC Certification Cost Breakdown by Expense Category Gap Assessment and Readiness Planning Costs A gap assessment maps your current environment against NIST SP 800-171 and typically costs $1,500 to $20,000 depending on depth and scope. This is the most valuable dollar you’ll spend in the entire project, because everything downstream is priced off what it finds. Documentation and System Security Plan (SSP) Costs The System Security Plan (SSP) is the cornerstone document of any assessment, mapping every control to your specific implementation. Professionally developed SSPs and supporting policies run $12,000 to $60,000. A weak SSP is one of the most common reasons assessments stall or fail, so this is a poor place to economize. Remediation and Security Control Implementation Costs Closing the gaps is usually the largest line item: $20,000 to $150,000 or more. Multi-factor authentication, logging and SIEM deployment, encryption, access control restructuring, and incident response capability all live here. Organizations with mature security postures spend far less than those starting from scratch. Technology and Infrastructure Upgrade Costs Many contractors move CUI into a dedicated enclave rather than securing their entire network. Enclave platforms typically cost $300 to $400 per user per month. Others upgrade endpoint protection, replace unsupported systems, or migrate to government-grade cloud environments, each with its own licensing and migration costs. C3PAO Assessment and Audit Fees The formal Level 2 assessment runs $30,000 to $100,000, driven by assessor-days, number of sites, and evidence quality. Well-organized evidence directly reduces assessor time and therefore your invoice. Consulting and Advisory Fees Specialist consultants, including Registered Practitioners (RPs) and

After a SOC 2 and ISO 27001 engagement, there are two documents out of the whole pile that actually close deals: the SOC 2 attestation report and the ISO 27001 certificate. Everything else your engagement produces exists to create those two, support them, or keep them alive for another year. Companies routinely ask their auditor for a SOC 2 certificate, which doesn’t exist. They send a prospect their full ISMS documentation when a one-page certificate would have done. They pay for six months of readiness work and then can’t say what they’re holding at the end of it. So here’s the full list. What a SOC 2 engagement produces, what an ISO 27001 engagement produces, what a combined program produces, and who gets to see each one. Understanding SOC 2 and ISO 27001 Engagement Outputs The Core Difference: Report vs. Certificate SOC 2 is an attestation. A licensed CPA firm examines your controls against the Trust Services Criteria under standards set by the AICPA, then writes up what it found and signs an opinion. No certificate. No logo from the AICPA. No pass or fail stamp. What you get is the report, and it usually runs 60 to 120 pages. ISO 27001 is a certification. An accredited certification body audits your Information Security Management System (ISMS) against ISO/IEC 27001:2022, and if you conform, it issues a certificate of registration. The certificate itself is a page or two. All the detail lives behind it, in your ISMS documentation and the audit reports the certification body writes as it goes. SOC 2 Engagement Deliverables The SOC 2 Attestation Report The report is the engagement. The AICPA’s illustrative SOC 2 report lays out the standard structure: auditor’s report, management’s assertion, system description, the Trust Services Criteria in scope, and the controls tested with their results. A Type I covers control design at one point in time. A Type II covers whether those controls actually operated over a period, usually three to twelve months, and most enterprise buyers now won’t accept anything else. Independent Auditor’s Opinion Letter First section of the report, and the first thing anyone experienced turns to. It gives the scope, the examination period, and the auditor’s conclusion. An unqualified opinion means the description held up and the controls worked. A qualified opinion means the auditor found something material, and every serious reviewer will want to talk about it. Management Assertion Your leadership signs a written statement stating that the system description is accurate and that the controls were properly designed and are operating. It reads like a formality, and it isn’t. The auditor’s entire examination runs against what management asserts here, so overstating anything creates real exposure. System Description Usually the longest part of the report, and you write it, not the auditor. It covers the services in scope, your infrastructure, software, people, processes, how data moves, which subservice organizations you depend on, and the complementary user entity controls your customers have to run on their side for your controls to hold up. Trust Services Criteria Applied Security (the Common Criteria) is in every SOC 2. Availability, Processing Integrity, Confidentiality, and Privacy are optional, and the report names exactly which ones you picked. Whatever you decide during scoping ends up printed in a document your customers read for the next several years. Description of Tests of Controls and Results (Type II) The matrix: every control, what the auditor did to test it, and what came back, including exceptions. Reviewers spend most of their time here, because the exceptions tell them things the opinion letter won’t. Bridge Letter / Gap Letter Your report covers a fixed window, so one ending December 31 leaves a hole for a customer doing diligence in June. A bridge letter from your management, not the auditor, confirms that nothing material changed in the control environment between the report’s end date and today. You’ll write these often enough to keep a template. Management Letter and Observations Plenty of auditors also send an internal-only letter covering observations, minor exceptions, and suggestions that never reached the threshold of a qualified opinion. It’s the closest thing to free consulting you’ll get before next year’s audit starts. Insider Note: Ask early whether your auditor issues a management letter, and whether exceptions land in the report body or only in that letter. Firms handle this differently, and the answer decides what your customers see versus what stays behind your firewall. It rarely comes up in the proposal, but it changes how the finished report reads to a buyer. ISO 27001 Engagement Deliverables ISO 27001 Certificate of Registration The document everyone asks for. It names the certified legal entity, states the ISMS scope, identifies the certification body, carries an accreditation mark from a body recognized under the International Accreditation Forum such as UKAS or ANAB, and shows the validity dates. It’s good for three years as long as you pass annual surveillance audits. Read the scope statement carefully, on your own certificate as much as anyone else’s. A certificate covering one office or one product line says nothing about the rest of the business. Statement of Applicability (SoA) After the certificate, this is the document buyers request most. The Statement of Applicability runs through all 93 Annex A controls in ISO/IEC 27001:2022, says which apply to you, justifies the ones you excluded, and records where each stands. Auditors use it as the map of your control environment, and larger customers increasingly want to see it or a summary of it during diligence. Risk Assessment and Risk Treatment Plan Your methodology, the register it produced, and the Risk Treatment Plan showing what you decided to do about each significant risk: mitigate it with a control, transfer it, avoid it, or accept it. ISO 27001 is built around risk, so these documents are what justify every control decision recorded in the SoA. Information Security Management System (ISMS) Documentation The policy and procedure set, plus the operational records that prove any of it happens. Information
The EU AI Act’s transparency requirements take effect on 2 August 2026, and most of the companies they cover still think the rules are not their problem. Article 50 applies to any business that publishes AI-generated content or runs an AI system that talks to people in the EU. That includes the marketing team generating campaign images and the support team running a chatbot. It also covers the AI agents you’ve wired into customer email. Penalties reach €15 million or 3% of total worldwide annual turnover, whichever is higher, and you don’t need an office in Europe to be in scope. If your content or your chatbot reaches EU users, the obligations reach you. In a nutshell: if you publish AI-generated images or video, deploy chatbots or AI agents that interact with EU users, or publish AI-written text on matters of public interest, then yes, the EU AI Act applies, starting 2 August 2026. A quick word on the “AI Act delay” headlines. The Digital Omnibus package did push the high-risk system deadlines back, in some cases by more than a year, but it did not move the deployer obligations in Article 50. Companies that read those headlines and stood down their AI Act work made an expensive mistake, because the rules most likely to touch an ordinary business are the ones that stayed on the calendar. What Article 50 Actually Requires Article 50 of the AI Act sets out transparency obligations in four situations. In plain English: Tell people when they’re talking to AI. Systems designed to interact directly with people — chatbots, voice assistants, and AI agents — must make clear that the user is dealing with AI, unless that’s already obvious. Mark AI-generated content so machines can detect it. Providers of generative AI systems must mark outputs in a machine-readable format, typically through metadata and watermarking, so the content is detectable as artificially generated. Label deepfakes. Anyone deploying AI to generate or manipulate image, audio, or video content that resembles real people, places, objects, or events, and could falsely appear authentic, must disclose that the content is artificial. Label AI-generated text on matters of public interest. Text published to inform the public must carry a label if AI-generated or manipulated, unless a human reviewed it and a person or organization holds editorial responsibility for it. Article 50 also covers emotion recognition and biometric categorization systems, which carry their own disclosure duties. Far fewer businesses run into those, so this article sticks to the four above. The distinction running through all of this is provider vs deployer. The provider builds or supplies the AI system. The deployer uses it professionally. Most companies reading this are deployers. If You Use AI-Generated Images Realistic AI images sit closer to the deepfake rules than most marketing teams assume. The Act’s definition covers content depicting people, objects, places, and events that could falsely appear authentic to a viewer, which describes a large share of what image generators produce for campaigns, social posts, and landing pages. So what does “clearly and distinguishably labeled” mean? The threshold is best described by its failures: a tiny disclosure hidden in the website footer doesn’t qualify. Neither does a faint label on an image, a label that flashes for an instant in a video, or a disclosure buried in your terms and conditions. The label has to be visible right where someone sees the content, and it has to meet accessibility standards so people with disabilities can perceive it too. The Code of Practice proposes a standardized “AI” visual label, localized per language (“KI” in German, “IA” in French). It also draws a useful line between fully AI-generated content and AI-assisted content, with lighter requirements for the latter. A designer who used AI to extend a background is in a different position from a team publishing a fully synthetic image of a person who doesn’t exist. Important: The deepfake duty doesn’t care about intent. A flattering, harmless AI image of your CEO at an event that never happened is still a deepfake under the Act. Marketing teams generate this kind of content casually. From August, every one of those images needs a label. If You Deploy AI Agents or Chatbots The rule itself is simple: people must know they’re dealing with AI. The provider carries the design obligation, but as the deployer you’re the one putting the system in front of your customers, and you’re the one an EU regulator will contact if your branded assistant pretends to be human. The Act contains an exception for cases where it’s “obvious” the user is talking to AI, judged from the perspective of a reasonably well-informed and observant person. Don’t lean on it. What’s obvious to your product team isn’t obvious to every customer, and the human-sounding voice agents and email-writing AI agents rolling out right now are designed specifically to not feel like software. If an AI agent negotiates a renewal over email or handles a support ticket end to end, disclose it. Pro Tip: Put the Disclosure at the Start of the Interaction Put the disclosure at the start of the interaction, in the interface itself: “You’re chatting with an AI assistant.” A line in your privacy policy doesn’t meet the standard, and a disclosure that appears after the conversation ends is worthless. For voice agents, say it up front in the greeting. What Your AI Vendors Owe You The machine-readable marking obligation in Article 50(2) sits with providers — the companies supplying your generative AI tools. The final Code of Practice expects providers to apply at least two layers of marking where necessary, such as embedded metadata combined with watermarking, and to offer detection mechanisms so deployers, authorities, and researchers can verify whether a piece of content came from AI. One timing caveat: the Digital Omnibus gives generative AI systems already on the market before 2 August 2026 until 2 December 2026 to comply with the marking requirement. Every other Article 50 obligation stays on

The CNIL‘s screening rule sounds simple: hit two of the nine high-risk criteria, and you owe a full Data Protection Impact Assessment (DPIA). The trouble starts when you hit one or none, because the GDPR never says that skipping the DPIA means skipping assessment altogether. Plenty of processing falls outside the CNIL’s screening rules: operations below the two-criteria threshold, activities on the CNIL’s exemption list, processing already covered by an earlier DPIA, and controllers who answer to a different supervisory authority altogether. In every one of those cases, the Article 35 GDPR DPIA obligation may fall away while the risk assessment obligations under Articles 24 and 32 stay exactly where they were. This article maps the scenarios where CNIL criteria don’t apply and what a defensible assessment strategy looks like when they don’t. DPIA vs General Risk Assessment: Core Distinctions Under GDPR These two assessments get conflated constantly, and the mix-up has real consequences. They rest on different legal bases, serve different purposes, and trigger under different conditions. Article 35 GDPR requires a DPIA where processing is “likely to result in a high risk” to people’s rights and freedoms, and it requires the assessment before processing begins. The DPIA looks outward. It evaluates the necessity and proportionality of the processing and the risks it creates for data subjects: discrimination, identity theft, financial loss, reputational damage, loss of control over personal data. The measuring stick throughout is harm to people. Article 32 GDPR requires controllers and processors to put in place technical and organizational measures (TOMs) appropriate to the risk of the processing. You can’t know what’s appropriate without assessing that risk first, so Article 32 carries an implicit risk assessment duty for every processing operation you run, high risk or not. Its focus is security: the confidentiality, integrity, availability, and resilience of the systems handling personal data. Article 24 completes the picture by making the controller responsible for implementing measures proportionate to risk and able to demonstrate compliance. That’s the accountability principle at work. So risk assessment is universal, and the DPIA is the escalated version you reserve for processing that crosses the high-risk line. The real question is which assessment to run and how deep to go. You don’t need a six-figure budget to be GDPR compliant. You need a clear plan and someone to do the work. Affordable GDPR Compliance Services Book a Free GDPR Consultation The CNIL Criteria: A Quick Recap The Article 35(3) Baseline and the 9 Criteria Article 35(3) names three situations where a DPIA is always mandatory: systematic and extensive automated evaluation of individuals, including profiling, with legal or similarly significant effects; large-scale processing of special categories of data (Article 9) or criminal conviction data (Article 10); and large-scale systematic monitoring of a publicly accessible area. Beyond those, the WP29 guidelines on DPIAs (WP248 rev.01), endorsed by the European Data Protection Board (EDPB), list nine criteria that indicate likely high-risk processing: evaluation or scoring, including profiling; automated decision-making with legal or similarly significant effect; systematic monitoring; sensitive data or data of a highly personal nature; processing on a large scale; matching or combining datasets; data concerning vulnerable data subjects (employees, patients, children); innovative use or application of new technological or organizational solutions; and processing that prevents data subjects from exercising a right or using a service or contract. The “Two Criteria” Threshold Rule The CNIL’s position is that processing meeting at least two of the nine criteria requires a DPIA as a general rule. WP248 leaves room on both sides of that line: a controller can conclude that processing meeting two criteria still isn’t high risk, and in some cases a single criterion is enough to trigger the obligation. Either way, the reasoning has to be documented. Where there’s genuine doubt, the CNIL’s advice is simple: do the DPIA. CNIL’s List of Processing Operations Requiring a DPIA The CNIL also maintains a mandatory list under Article 35(4), adopted through Deliberation No. 2018-327 of October 11, 2018. It names 14 types of processing that require a DPIA outright, including systematic employee monitoring, whistleblowing schemes, profiling that can exclude people from a contract, and large-scale processing of health data. If your processing appears on this list, you can skip the criteria math because the DPIA is mandatory regardless. Insider Note: The CNIL’s sectoral “referentials” do more work than most DPOs realize. If your processing fully complies with an applicable referential, the CNIL accepts the position that residual risk isn’t high, which takes Article 36 prior consultation off the table. Checking for a referential before scoping a DPIA can remove the most painful step of the entire process. When CNIL Criteria Don’t Apply: Key Scenarios Processing Falling Below the Two-Criteria Threshold Most B2B processing lives here. A standard CRM, a newsletter list, routine supplier management: these might touch one criterion (large scale, perhaps) without hitting a second. No DPIA is required, but the screening itself is a compliance artifact. Record which criteria you tested, what you concluded, and why. If the CNIL inspects, the absence of a DPIA is defensible only when the screening decision is on paper. Operations on CNIL’s Exemption List Article 35(5) lets supervisory authorities publish “whitelists” of processing that doesn’t require a DPIA. The CNIL adopted one in 2019 after an EDPB opinion, covering categories such as routine HR management in organizations with fewer than 250 employees (without profiling, biometrics, or sensitive data), badge-based physical access control without biometrics, and time management systems that don’t process biometric data. France is one of only a few member states with a formal whitelist, which matters for cross-border groups: the same HR system can be exempt in France and assessable case by case in Luxembourg. Processing Authorized by Specific Legal Provisions Article 35(10) carves out processing based on a legal obligation or public interest task under Article 6(1)(c) or (e), where the legal basis regulates the specific operation and a general impact assessment was already carried out when that law was adopted. It’s a narrow
Only one of these three vendors sells a FedRAMP-authorized identity platform you can buy today as a defense contractor, one sells two of them, and one sells none. Whether that matters for your CMMC Level 2 assessment depends entirely on whether your identity provider stores, processes, or transmits Controlled Unclassified Information (CUI), or provides security protections for the systems that do. That second condition is where most contractors get the analysis wrong. The IdP question is arguably the most argued-about scoping decision in CMMC 2.0 Level 2 preparation, because an identity provider almost never holds CUI directly, yet it controls access to everything that does. This article works through the regulatory requirement, the actual FedRAMP status of JumpCloud, Okta, and Microsoft Entra ID, and how to choose based on your CUI architecture rather than vendor marketing. Understanding the CMMC Level 2 + FedRAMP Requirement What CMMC Level 2 Requires for Cloud Services Handling CUI CMMC 2.0 Level 2 requires contractors to implement the 110 security requirements of NIST SP 800-171 Rev. 2 and, for most contracts, pass a third-party assessment by a Certified Third-Party Assessor Organization (C3PAO). The 48 CFR acquisition rule took effect on November 10, 2025, which means CMMC clauses now appear in new Department of Defense (DoD) solicitations, with third-party assessment requirements expanding through the phased rollout in 2026 and beyond. The cloud piece comes from the CMMC program rule at 32 CFR Part 170. If an Organization Seeking Certification uses a Cloud Service Provider (CSP) to process, store, or transmit CUI, that cloud service offering must be either FedRAMP Authorized at the Moderate baseline or higher or must meet security requirements equivalent to the FedRAMP Moderate baseline. Your C3PAO verifies this during the assessment. If your in-scope CSP fails the test, you fail the assessment. The DFARS 252.204-7012 “FedRAMP Moderate or Equivalent” Clause The requirement predates CMMC. DFARS 252.204-7012 has required since 2016 that any external CSP used to store, process, or transmit covered defense information meet security requirements “equivalent to those established by the Government for the Federal Risk and Authorization Management Program (FedRAMP) Moderate baseline.” For years, “equivalent” was undefined, and contractors interpreted it loosely. The DoD CIO closed that door with its December 2023 equivalency memo. To be FedRAMP Moderate Equivalent, a CSP must now demonstrate 100% compliance with the FedRAMP Moderate baseline, validated by a FedRAMP-recognized Third-Party Assessment Organization (3PAO), and hand over a full Body of Evidence to the contractor. No open Plans of Action and Milestones (POA&Ms) against the baseline are permitted. In some ways, it’s stricter than authorization itself, since authorized CSPs are allowed to carry POA&Ms. Important: A vendor telling you they are “NIST 800-171 compliant” or “aligned to FedRAMP controls” does not satisfy DFARS 7012 or the CMMC rule. Either the offering appears on the FedRAMP Marketplace at Moderate or higher, or the vendor gives you a 3PAO-attested Body of Evidence demonstrating full equivalency. Anything else is a gap your C3PAO will find. When an Identity Provider Falls Under This Requirement An IdP is a cloud service. The question is whether it processes, stores, or transmits CUI. In a typical SSO flow, the IdP handles credentials, authentication tokens, session data, and directory attributes. None of that is CUI in most environments. So a literal reading says the FedRAMP mandate doesn’t apply. The complication is the CMMC scoping guidance, which defines Security Protection Assets (SPAs): assets that provide security functions to the CMMC assessment scope even if they never touch CUI. An IdP enforcing multi-factor authentication (MFA), conditional access, and session policy over your CUI enclave is the textbook SPA. SPAs are in scope for your assessment and get evaluated against the relevant NIST SP 800-171 requirements they help satisfy. Let Axipro help you build a business continuity plan that’s practical, compliant, and audit-ready. Schedule Your Free Assessment Today Schedule A Consultation Does Your Identity Provider Actually Need to Be FedRAMP Authorized? When the IdP Processes, Stores, or Transmits CUI Some architectures do push CUI through the identity layer. If usernames or directory attributes contain CUI (think program names or export-controlled project identifiers), if your IdP proxies application traffic through a gateway that carries CUI payloads, or if CUI-bearing documents get attached to identity workflows, the IdP is now a CSP handling CUI. FedRAMP Moderate or equivalent becomes non-negotiable. When the IdP Provides Security Protections for CUI (SPA Role) This is the common case, and it’s genuinely gray. The FedRAMP requirement in the rule text attaches to CSPs that process, store, or transmit CUI. A pure-play authentication service that does neither is an SPA, not a CUI-handling CSP. Under the final CMMC rule, External Service Providers (ESPs) that handle only Security Protection Data, such as configuration data, logs, and credentials, do not themselves require FedRAMP authorization or a separate CMMC certification. Their services get assessed as part of your assessment. In practice, C3PAOs are not uniform on this. Some accept a well-documented System Security Plan (SSP) showing the IdP never touches CUI. Others take a conservative view that authentication data for CUI systems is sensitive enough that they want FedRAMP-grade assurance behind it, and they will probe hard. DIBCAC’s historical position, given publicly by officials as far back as 2020, is that clouds with management access to CUI systems don’t need FedRAMP unless CUI actually moves into them. That position helps, but you carry the burden of proving CUI never transits the service. Cases Where a Commercial IdP May Be Acceptable A commercial, non-FedRAMP IdP can survive a CMMC Level 2 assessment when all three of the following are true: CUI demonstrably never touches the IdP, the IdP is documented as an SPA with the specific 800-171 requirements it supports, and the data flows in your SSP prove the boundary. This is exactly how many contractors run enclave strategies, keeping a commercial identity stack for the corporate network while the CUI enclave uses its own FedRAMP-authorized identity. The “External Service Provider” (ESP) Classification Under CMMC The final

An AI agent that can read your inbox, query your CRM, and dig through internal documents has more standing access than most of your employees. It handles sensitive data, acts on its own, and often passes that data through sub-processors you’ll never see. Certifications are the quickest way to tell which vendors have let an outsider check their work, and which ones just put the word “secure” on a landing page. No single certificate proves an AI agent is safe. But the right mix of security attestations, privacy certifications, and AI governance standards tells you the vendor has real controls, that an independent auditor has tested them, and that someone is on the hook when the agent misbehaves. This guide covers which certifications to ask for, how to verify them, and which claims should make you walk away. The Core Certifications Every Secure AI Agent Vendor Should Hold SOC 2 Type II SOC 2 Type II is the baseline for any SaaS or AI vendor that handles customer data. A licensed CPA firm audits the vendor against the AICPA’s Trust Services Criteria (Security, Availability, Processing Integrity, Confidentiality, and Privacy) and reports on whether its controls actually worked over a review period, usually 3 to 12 months. A Type I report only confirms the controls existed on one particular day. For an AI agent vendor, insist on Type II. Anything less tells you nothing about how the company runs day-to-day. ISO/IEC 27001 ISO/IEC 27001 certifies that the vendor runs a formal information security management system (ISMS): documented risk assessments, defined controls, internal audits, and management review, all verified by an accredited certification body. It’s the most widely recognized security certification outside the US and often a hard procurement requirement in Europe, the UK, and the Gulf. A vendor with international customers should hold it alongside SOC 2, not instead of it. ISO/IEC 27701 (Privacy Information Management) ISO/IEC 27701 extends ISO 27001 with a privacy information management system (PIMS). It maps closely to GDPR concepts like controller and processor obligations, consent, and data subject rights. Almost every AI agent processes personal data at scale, and ISO 27701 is a decent signal that the vendor has built privacy into how it operates instead of delegating it to a policy PDF. ISO/IEC 42001 (AI Management Systems) ISO/IEC 42001 is the first certifiable international standard for AI governance. According to the International Organization for Standardization, it sets out requirements for building and maintaining an AI management system (AIMS): AI risk management, AI system impact assessments, lifecycle management, and oversight of third-party suppliers. For an AI agent vendor, this is the one that covers what SOC 2 and ISO 27001 don’t: how the vendor governs model behavior, training data, and the wider impact of autonomous systems. Worth Knowing: ISO 42001 certificates only started appearing in volume in 2024, and the accreditation ecosystem is still catching up. Check that the certificate came from a certification body accredited for ISO 42001 specifically (under ANAB or UKAS, for example), not just one accredited for ISO 27001. HIPAA (for Healthcare AI Agents) If the agent touches protected health information (PHI), the vendor has to comply with the HIPAA Privacy and Security Rules and sign a Business Associate Agreement (BAA). There’s no official HIPAA certification, so vendors prove compliance through third-party assessments, a SOC 2 with HIPAA mapping, or HITRUST CSF certification. A vendor that won’t sign a BAA has disqualified itself for healthcare work. PCI DSS (for Payment-Handling AI Agents) AI agents that process, store, or transmit cardholder data (think agents automating billing, refunds, or checkout) fall under PCI DSS. Ask for the vendor’s Attestation of Compliance (AOC) and check whether a Qualified Security Assessor validated it or the vendor assessed itself. The current version is PCI DSS 4.x, so an AOC that still references 3.2.1 is out of date. FedRAMP (for Government-Facing AI Agents) FedRAMP authorization is mandatory for cloud services sold to US federal agencies. Authorizations come at Low, Moderate, and High impact levels, and every authorized service appears on the public FedRAMP Marketplace. If a vendor claims FedRAMP status and isn’t in the Marketplace, either the claim is false or the service is still “in process,” and those are very different things. State and local buyers should look for StateRAMP instead. Worth Knowing: ISO 42001 Certificates ISO 42001 certificates only started appearing in volume in 2024, and the accreditation ecosystem is still catching up. Check that the certificate came from a certification body accredited for ISO 42001 specifically (under ANAB or UKAS, for example), not just one accredited for ISO 27001. HIPAA (for Healthcare AI Agents) If the agent touches protected health information (PHI), the vendor has to comply with the HIPAA Privacy and Security Rules and sign a Business Associate Agreement (BAA). There’s no official HIPAA certification, so vendors prove compliance through third-party assessments, a SOC 2 with HIPAA mapping, or HITRUST CSF certification. A vendor that won’t sign a BAA has disqualified itself for healthcare work. PCI DSS (for Payment-Handling AI Agents) AI agents that process, store, or transmit cardholder data (think agents automating billing, refunds, or checkout) fall under PCI DSS. Ask for the vendor’s Attestation of Compliance (AOC) and check whether a Qualified Security Assessor validated it or the vendor assessed itself. The current version is PCI DSS 4.x, so an AOC that still references 3.2.1 is out of date. FedRAMP (for Government-Facing AI Agents) FedRAMP authorization is mandatory for cloud services sold to US federal agencies. Authorizations come at Low, Moderate, and High impact levels, and every authorized service appears on the public FedRAMP Marketplace. If a vendor claims FedRAMP status and isn’t in the Marketplace, either the claim is false or the service is still “in process,” and those are very different things. State and local buyers should look for StateRAMP instead. Regulatory Frameworks AI Agent Vendors Must Comply With Certifications are voluntary. Regulations aren’t. A credible AI agent vendor should be able to explain, in writing, how it meets

One in five organizations has already suffered a breach traced back to shadow AI. Meanwhile, 63% of breached organizations either have no AI governance policy at all or are still drafting one. Below is a complete, copy-ready shadow AI policy template with twelve sections, plus guidance on adapting it for your company size, your industry, and the regulatory frameworks you answer to. The template assumes one hard truth up front: your employees are already using unapproved AI tools. A policy that pretends adoption hasn’t started yet fails on day one, so this one starts from the assumption that it has. What Is a Shadow AI Policy? A shadow AI policy is a formal document that defines how your organization discovers, evaluates, approves, and governs AI tools that employees adopt outside official IT channels. The term borrows from shadow IT, the older problem of unsanctioned software and hardware, but the AI version carries sharper risks: data pasted into a public model may be retained, used for training, or exposed in ways the organization can’t reverse. The policy does three jobs: it separates approved use from unapproved use, gives employees a fast and visible way to request new tools so the sanctioned route beats the workaround, and spells out what happens when someone crosses the line, including how the organization detects it and responds. Shadow AI Policy vs. General AI Acceptable Use Policy Many organizations already have an AI acceptable use policy (AUP) and assume it covers shadow AI. It usually doesn’t. An AUP tells employees how to behave inside approved tools. A shadow AI policy governs the tools themselves: which ones exist in your environment, which ones are allowed, and what happens with the rest. You need both. The AUP handles conduct; the shadow AI policy handles inventory and control. If you only have room for one document, fold the AUP’s data-handling rules into Section 6 of the template below. The Shadow AI Policy Template (Download Link and Copy-Ready Sections) We’ve created a compliance safe template for Shadow AI Policy, use the link below to create a copy and customize for your company: Download The Shadow AI Policy Template → Copy the sections below into your policy management system and replace the bracketed placeholders. The language is plain on purpose. Legalese gets skimmed. Section 1: Purpose and Scope This policy governs the acquisition, approval, and use of artificial intelligence tools, features, and services at [Company]. It applies to all employees, contractors, interns, and third parties with access to [Company] systems or data. It covers standalone AI applications, AI features embedded in existing software, browser extensions, AI agents, APIs, and personal AI accounts used for work purposes, on both corporate and personal devices. The purpose of this policy is to enable productive AI use while protecting [Company] data, customers, and legal obligations. This policy does not prohibit AI. It prohibits ungoverned AI. That last sentence matters. Employees read the purpose statement first, and it decides whether they see the policy as an enabler or a blocker. Section 2: Definitions and Terminology Shadow AI: any AI tool, feature, agent, or service used for work purposes without formal approval under this policy. Approved AI Tool: an AI tool listed in the Approved AI Tools Registry (Section 4) and used under a [Company]-managed account. Personal AI Account: an account on any AI service registered to a personal email address or paid for personally. AI Feature: AI functionality embedded within otherwise approved software (e.g., an AI assistant added to a project management tool), which requires separate evaluation. Sensitive Data: data classified as [Confidential] or [Restricted] under [Company]‘s data classification policy, including the prohibited data classes in Section 6. Define “AI feature” explicitly. Vendors now ship AI additions into already-approved SaaS products every month, and without this definition, those features inherit approval they never earned. Section 3: Roles and Responsibilities The CISO (or designated security lead) owns this policy, maintains the Approved AI Tools Registry, and runs the approval workflow. Department heads ensure their teams know the policy and surface tool requests rather than suppressing them. Legal and Compliance review tools that touch regulated data or fall under the EU AI Act, GDPR, HIPAA, or client contractual restrictions. IT operates detection and monitoring controls (Section 9). Every employee is responsible for using only approved tools for work, reporting unapproved AI use they discover, and requesting new tools through the workflow in Section 7 rather than adopting them directly. Insider Note: In organizations under roughly 200 people, the “CISO” in this section is often the same overworked IT lead who manages laptops. Name a real person, not a title that doesn’t exist yet. A policy that assigns duties to a phantom role is unenforceable, and auditors notice. Section 4: Approved AI Tools Registry [Company] maintains a registry of approved AI tools at [location/URL]. For each tool, the registry records: tool name and vendor, approved use cases, prohibited use cases, permitted data classes, account type (enterprise/team/individual), data retention and training settings, risk tier (Section 5), approval date, and next review date. Only tools listed in the registry may be used for work. Tools not listed are unapproved by default. The registry is reviewed [quarterly]. Keep the registry somewhere employees actually look, such as your intranet homepage or IT help center, not buried in a GRC platform they can’t access. An invisible registry recreates the problem the policy exists to fix. Section 5: Risk Tier Classification (Low, Medium, High) Each tool in the registry is assigned a risk tier. Low: the tool processes only public or internal non-sensitive data, runs under an enterprise agreement with training opt-out, and produces output that a human reviews before use. Approval by IT Security alone. Medium: the tool processes internal business data or connects to [Company] systems via API or integration. Approval by IT Security plus the data owner. High: the tool processes sensitive data, customer personal data, or regulated data; makes or influences consequential decisions (hiring, credit, medical, legal); or operates autonomously
Legacy threat modeling frameworks such as STRIDE were designed for software that behaves the same way over and over again. Agentic AI does no such thing. It can rewrite its own plan mid-task, call external tools, negotiate with other agents, and produce a different output from identical input. MAESTRO exists because none of the legacy threat modeling frameworks were built to handle that. MAESTRO stands for Multi-Agent Environment, Security, Threat, Risk, and Outcome. It is a seven-layer threat modeling framework created specifically for agentic AI systems, and it has become the closest thing the industry has to a standard method for reasoning about agent security. Understanding MAESTRO in the Context of Agentic AI What MAESTRO Stands For Each word in the acronym carries meaning. Multi-Agent Environment signals that the framework models entire ecosystems of interacting agents, not a single model behind an API. Security, Threat, Risk covers the core discipline: identifying attack surfaces, cataloging threats, and assessing likelihood and impact. Outcome is the part most frameworks skip. MAESTRO asks what an attack actually produces in the real world, because an autonomous agent with tool access turns a compromised prompt into a compromised action. The Origin of MAESTRO (Cloud Security Alliance) The Cloud Security Alliance published MAESTRO in February 2025. Its creator is Ken Huang, Co-Chair of the CSA AI Safety Working Groups and CEO of DistributedApps.ai. The CSA has since applied the framework publicly to real systems, including OpenAI’s Responses API and Google’s A2A protocol, which gives practitioners worked examples rather than just theory. The framework is openly published, and the CSA maintains an official companion tool, the MAESTRO Threat Analyzer, on GitHub. SOC 2, ISO 27001 and HIPAA done for you. Fixed fee, 100% audit pass rate. Audit-ready in 6 weeks. Not 6 months. Schedule Free Assessment Why Traditional Frameworks Fall Short for Agentic AI STRIDE, PASTA, LINDDUN, and OCTAVE all share a founding assumption: the system under analysis follows predictable logic with clearly defined boundaries. You draw the data flow diagram, mark the trust boundaries, and enumerate threats against components that behave deterministically. Agentic AI breaks every part of that assumption. Unique Security Challenges of Autonomous Agents Agents introduce three properties that legacy models cannot express. Non-determinism means the same input can produce different behavior, so you cannot enumerate execution paths in advance. Autonomy means the agent makes decisions and takes actions without a human approving each step, which collapses the usual assumption that a person sits between intent and execution. And in multi-agent systems there is often no stable trust boundary: agents delegate to other agents, consume tool outputs from external servers via protocols like the Model Context Protocol (MCP), and update their own memory and goals at runtime. The Gap Between Legacy Frameworks and Agent-Based Systems The practical consequence is coverage gaps. STRIDE has no category for goal manipulation, where an attacker gradually steers what an agent is trying to achieve. PASTA assumes attacker objectives and data flows are fixed, which fails for systems that learn and adapt during operation. LINDDUN addresses privacy but says nothing about agent collusion or memory poisoning. A threat model built purely on these frameworks will pass review and still miss the attacks that matter most in an agentic deployment. How MAESTRO Addresses Agentic-Specific Risks MAESTRO does not discard the older frameworks. It extends them with a layered reference architecture, an AI-specific threat catalog for each layer, and, critically, explicit analysis of how threats propagate between layers. That cross-layer lens is the framework’s real contribution, because most serious agentic incidents are chains: poisoned data influences a model, the model misleads an agent, and the agent takes an unauthorized action three layers away from where the attack started. The Seven Layers of the MAESTRO Framework MAESTRO decomposes any agentic system into seven layers, each with its own threat landscape. Layer 1: Foundation Models The core LLMs or other models the agents reason with. Threats here include adversarial examples, model extraction, backdoored weights, and jailbreaks that bypass safety training. If the model is a third-party API, supply chain risk lives at this layer too. Layer 2: Data Operations Everything the agent ingests, stores, and retrieves: training data, RAG pipelines, vector databases, and agent memory. Data poisoning and memory tampering are the signature threats at this layer, and they are especially dangerous because a poisoned memory persists across sessions and keeps shaping future decisions long after the initial attack. Layer 3: Agent Frameworks The orchestration software that turns a model into an agent: LangChain, CrewAI, AutoGen, custom planners, and tool-calling logic. Threats include prompt injection through tool outputs, insecure tool definitions, and manipulation of the planning loop itself. Layer 4: Deployment Infrastructure The servers, containers, and cloud services the agents run on. The CSA’s threat catalog here reads like traditional cloud security with an agentic twist: compromised container images carrying malicious agent code, Kubernetes orchestration attacks, denial of service against agent runtimes, and tampering with Infrastructure-as-Code templates that provision agent resources. Layer 5: Evaluation and Observability The systems that monitor, evaluate, and debug agent behavior. This layer is often forgotten, and attackers know it. The CSA specifically flags poisoning observability data: manipulating the telemetry fed to monitoring systems so that incidents stay hidden from security teams while malicious activity continues. Layer 6: Security and Compliance MAESTRO treats this as a vertical layer that cuts across all others: identity and access management, guardrails, policy enforcement, and compliance controls. Threats include permission escalation, guardrail bypass, and compromise of the security agents themselves in architectures where AI enforces policy on other AI. Layer 7: Agent Ecosystem The environment where agents interact with users, other agents, and marketplaces. This is where the genuinely novel threats live: agent impersonation, misleading agent capability cards, tool squatting, and collusion between agents to achieve outcomes no single agent was authorized to pursue. Insider Note: In real assessments, Layers 5 and 6 expose the maturity gap fastest. Most teams’ shipping agents can describe their model and their orchestration framework in detail, then
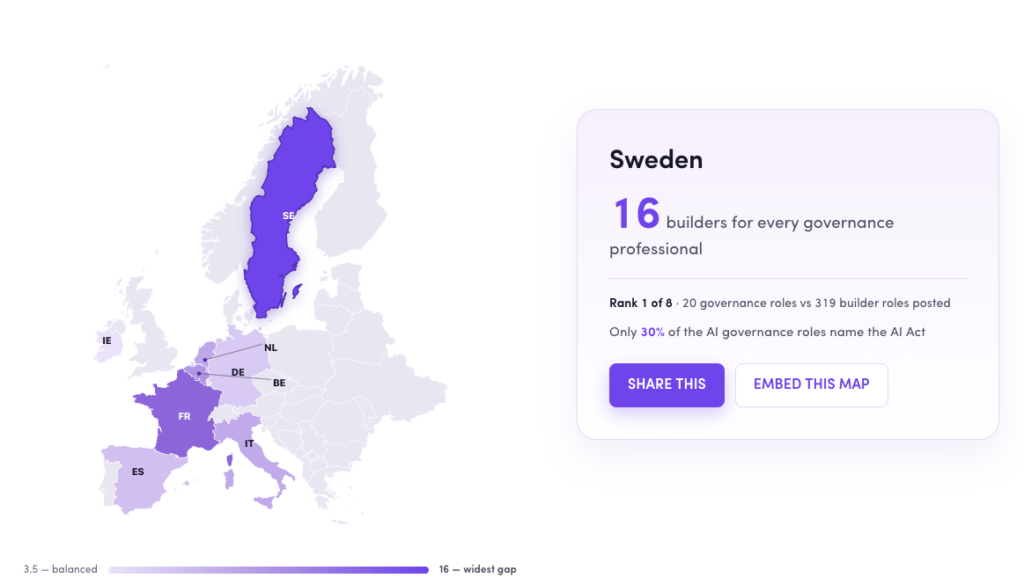
AXIPRO STUDY New Study: Europe is hiring AI builders faster than AI governance professionals Axipro analyzed 3,519 AI-related job postings across eight EU countries. For every professional hired to keep AI lawful, safe and accountable, nearly seven were hired to build more of it, and the gap is widest exactly where you’d least expect. Take EU AI ACT READINESS QUIZZ 16 AI Builders : 1 AI Governors Sweden — Europe’s widest AI governance gap 3,519 Job Postings Analyzed 8 EU Countries 2 Role Categories: Builders vs Governors July 2026 Date of Job Postings Analyzed The findings Finding 1: Sweden hires 16 AI builders for every 1 person to govern them Throughout our data-set we found the same pattern across all eight countries: the more a nation hires to build AI, the less it hires to govern it. France runs eleven builders to every governor. Even Ireland, the most balanced in Europe, looks responsible mainly because the US tech giants headquartered there import global-governance discipline under overlapping DORA and AI Act pressure. 3.5→16 builders hired per governor, Europe’s most balanced country to its least. Ireland 3.5 Germany 5.7 Spain 6.0 Italy 7.1 Netherlands 7.2 Belgium 7.9 France 11.4 Sweden 16:1 0 4 8 12 16 Builders hired per AI governor Source: Axipro, 2026 Sweden has one of the strongest engineering cultures in Europe. It also carries the widest governance gap we measured: sixteen AI builders hired for every person hired to govern them. France sits close behind at eleven to one. The most balanced country, Ireland at 3.5 to one, looks responsible for a reason that has little to do with virtue. The US tech giants headquartered in Dublin import global governance discipline, and they do it under the combined weight of the AI Act and DORA, the EU financial-sector resilience regime in force since January 2025. Engineering strength does nothing to close a governance gap, and it may widen it. A country that ships AI faster produces more systems that fall under the Act’s scope and, on this evidence, fewer people positioned to document, monitor, and defend them. Being good at building AI offers no protection against governing it badly. The countries most confident in their technical talent are running the largest deficit against the law. Explore AI governance hiring by country Click any country to see how many AI builders it hires for every governance professional, and where it ranks against the rest of Europe. Germany — 5.7 builders per governorDE France — 11.4 builders per governorFR Spain — 6.0 builders per governorES Italy — 7.1 builders per governorIT Netherlands — 7.2 builders per governorNL Belgium — 7.9 builders per governorBE Ireland — 3.5 builders per governorIE Sweden — 16 builders per governorSE 3.5 — balanced 16 — widest gap Source: Axipro, 2026 Sweden 16builders for every governance professional Rank 1 of 8 · 20 governance roles vs 319 builder roles posted Only 30% of the AI governance roles name the AI Act Share this Embed this map Copy & paste — links back to Axipro Copy embed code Branded, one paste, backlink included. × Share this country insight Share this AI governance gap X / Twitter LinkedIn Facebook WhatsApp Bluesky Email Copy link Choose a platform or copy the link. A view of the same country-level dataset behind the interactive map: governance roles, builder roles, builder-to-governance ratio, and the share of governance postings that name the EU AI Act. AI governance jobs Europe statistics by country: governance roles, builder roles, builder-to-governance ratio and AI Act mention percentage. Country Governance roles Builder roles Builder-to-governance ratio AI Act mention % Sweden 20 319 16.0:1 30.0% France 39 443 11.4:1 38.5% Belgium 38 299 7.9:1 39.5% Netherlands 61 439 7.2:1 31.1% Italy 40 284 7.1:1 45.0% Spain 64 384 6.0:1 28.1% Germany 88 501 5.7:1 27.3% Ireland 96 335 3.5:1 14.6% Source: Axipro analysis of AI builder, governance and compliance job postings across eight European countries. “AI Act mention %” is the share of governance postings that explicitly name the EU AI Act. Finding 2: The law nobody names. Most AI governance jobs still do not mention the EU AI Act Europe spent years drafting the AI Act. It cleared the European Parliament, survived the Digital Omnibus revisions, and now carries penalties that reach €35 million or 7% of global turnover for the most serious breaches, a ceiling that makes GDPR fines look modest. Yet fewer than three in ten of the governance roles created to handle it actually name the law in the job description. Among builder roles, the figure collapses to one in twenty-five. More than 7 in 10 Governance job descriptions do not mention the EU AI Act. This number rises to 9 in 10 for all AI job descriptions. Despite hiring for governance, risk, privacy, and compliance roles, most employers are not yet translating the EU AI Act into explicit job requirements. That disconnect should stop you. The people being hired to make Europe compliant are, for the most part, not being hired against the Act by name. They are titled around adjacent ideas: risk, ethics, model validation, data protection. Some of that work will map onto the Act’s requirements. Much of it will not, because a role written without the regulation in view rarely produces the conformity assessments, technical documentation, and human-oversight structures the Act specifically demands. Readiness is even thinner than the headcount suggests. Simply counting governance hires overstates how many people are actually working the law. What job descriptions actually name The EU AI Act is visible in governance roles — but still absent from most job ads. Across the laws and frameworks most relevant to AI governance hiring, the EU AI Act appears in fewer than three in ten governance postings, and only 4% of builder postings. Law or framework Governance roles naming it Builder roles naming it All roles naming it Governance mentions EU AI Act 28.5% 4.0% 7.6% 127 GDPR 26.9% 5.7% 9.6% 120 ISO 27001 11.4% 1.3% 2.8% 51
Compliance Hubs
Discover key insights, educational articles, helpful guides and more.
Most organizations think their AI governance is further along than it is. McKinsey’s 2026 AI Trust Maturity Survey of roughly 500 organizations found an average maturity score of 2.3 out of 4, and only about a third reported level three or higher in strategy, governance, and agentic AI oversight. Adoption is outpacing control, and regulators have noticed. An AI governance maturity model gives you a way to measure that gap honestly. This guide covers what a maturity model is, the six dimensions it should measure, the five levels most models use, and how to assess your own organization and build a roadmap to the next level. What Is an AI Governance Maturity Model? An AI governance maturity model is a structured framework that describes how capable an organization is at governing its AI systems, usually across five progressive levels. The concept borrows directly from the Capability Maturity Model (CMM) that software engineering has used since the early 1990s: define the capability, describe what it looks like at each stage of development, and score yourself against it. The purpose is diagnosis. A maturity model tells you where governance is strong, where it’s theater, and where it doesn’t exist at all. How It Differs from General AI Governance Frameworks Frameworks like the NIST AI Risk Management Framework or ISO/IEC 42001 tell you what good governance contains: policies, risk assessments, accountability structures, monitoring. A maturity model tells you how well you’re doing those things today. The framework is the destination. The maturity model is the odometer. That distinction matters in practice. Plenty of companies can point to an AI policy document. Far fewer can show that the policy changes what teams actually ship. Why Enterprises Need a Maturity Model Three reasons. First, budget: you can’t prioritize governance investment without knowing which dimension lags. Second, accountability: a maturity score gives boards something concrete to track quarter over quarter. Third, regulation: the EU AI Act and frameworks like ISO 42001 assume a functioning management system, and a maturity assessment is the fastest way to find out whether yours would survive scrutiny. Core Dimensions of an AI Governance Maturity Model A useful model measures more than policy coverage. Six dimensions show up consistently across the credible models, including the IEEE-USA flexible maturity model built on the NIST AI RMF. Strategy and leadership. Does the organization have a stated position on AI risk, an executive owner (increasingly a Chief AI Officer), and board visibility? Gartner’s 2025 polling found 55% of organizations now have an AI board or dedicated oversight committee, which means nearly half still govern by improvisation. Policies, standards, and accountability. Written policies mapped to regulations, a RACI matrix for AI decisions, and clear escalation paths. Many organizations adapt the three lines of defense model from financial risk: the teams building AI, the risk function overseeing them, and internal audit checking both. Data governance and model lifecycle. Training data lineage, quality controls, and lifecycle management from development through deployment, monitoring, and retirement. This is where AI governance meets MLOps, and where mature organizations maintain an AI register, a live inventory of every model and system in production. Risk, compliance, and ethics. Risk classification of AI systems, impact assessments, bias and fairness testing, and explainability requirements. Banks will recognize the DNA of model risk management under SR 11-7 here. People, skills, and culture. Training, role clarity, and whether people outside the governance team actually understand their obligations. Tools, automation, and monitoring. Drift detection, automated policy checks, audit logging, and dashboards. Governance that lives in spreadsheets caps out around level three. The 5 Levels of AI Governance Maturity Level 1: Ad Hoc / Initial AI use happens without oversight. There’s no inventory, no policy, or a policy nobody follows. Shadow AI is common, and risk surfaces only when something breaks publicly. Level 2: Developing / Repeatable Someone has been assigned responsibility. A draft policy exists, a partial inventory exists, and reviews happen for high-profile projects. The practices are repeatable but depend on specific people rather than defined processes. Level 3: Defined / Structured Governance is documented, standardized, and applied across the organization. There’s a governance committee, a risk classification scheme, defined lifecycle gates, and mandatory training. Most organizations pursuing ISO 42001 certification are working to reach and formalize this level. Level 4: Managed / Metrics-Driven Governance produces numbers. Coverage rates, review cycle times, incident counts, and risk reduction are measured and reported to leadership. Controls are enforced by tooling rather than goodwill, and audits confirm the system works as described. Level 5: Optimized / Adaptive Governance improves itself. Monitoring feeds back into policy, controls adapt to new model types (agentic systems being the current test), and the organization anticipates regulatory change rather than reacting to it. Almost nobody is here yet, and that’s fine. Level 5 is a direction, not a deadline. Insider Note: In assessments, the most common self-scoring error is claiming level 3 on the strength of documents alone. If your policy says every model gets a pre-deployment review and your inventory shows 40 models but your review log shows 6, you’re at level 2. Evidence beats paperwork every time, and auditors check the logs first. AI Governance Maturity Matrix The matrix crosses dimensions with levels so you can score each one independently. Organizations are rarely uniform: it’s normal to sit at level 3 on policy and level 1 on monitoring. For scoring, keep the rubric simple: 1 to 5 per dimension, scored on evidence you could show an auditor, not on intentions. Board-level indicators (does the board see AI risk reporting?) and operational indicators (does every production model have a completed impact assessment?) should be scored separately, because they fail independently. How to Assess Your Current AI Governance Maturity Start with a baseline self-assessment. Pull together a cross-functional group covering engineering, legal, risk, security, and the business owners of major AI use cases, and score each dimension against the matrix. Half a day is usually enough for a first pass. For each dimension, the
Most organizations get ISO 42001 certified in 2 to 9 months. Companies that already hold ISO 27001 regularly land in the 2 to 5 month range, while enterprises with sprawling AI portfolios and no existing management system can take 12 months or more. The audit itself only takes days. Almost the entire calendar goes into building and operating your AI Management System (AIMS) long enough to produce evidence an auditor can actually check. That is the short answer. The longer answer depends on your starting point, your scope, and how quickly you can get a certification body on the schedule. This article breaks down the full timeline phase by phase, the factors that stretch or compress it, and what the recertification cycle looks like once you hold the certificate. Typical ISO 42001 Certification Timeline at a Glance ISO/IEC 42001:2023 is the first international standard for AI management systems, published in December 2023. Because it follows the same harmonized structure as ISO 27001 and ISO 9001, the certification process will feel familiar to anyone who has been through a management system audit: build the system, run it, pass a Stage 1 and Stage 2 audit, then maintain it through annual surveillance. Here is how timelines typically break down by company size. Average Timeline for Small Businesses Small companies move fastest because scope stays contained. A startup with two or three AI systems, a handful of decision makers, and short approval chains can finish scoping in a week and get policies signed off in days rather than weeks. The realistic floor for a small business starting from scratch is around 3 months. With an existing ISO 27001 program and a compliance platform already collecting evidence, 2 months is achievable. Average Timeline for Mid-Sized Companies Mid-sized companies usually take 6 to 9 months. The AI inventory is growing, more departments are touching AI systems, and risk assessments have to cover more use cases. Coordination becomes the hidden cost: getting engineering, legal, and product to agree on an AI policy takes longer than writing the policy itself. Average Timeline for Enterprises Enterprises should plan for 9 to 12 months, sometimes longer. The main drivers are AI system sprawl across business units, longer procurement cycles for certification bodies, and audits that take more days. The Stage 2 audit for a large multinational can run two weeks or more on its own, and internal alignment before the audit takes far longer than the audit itself. Breakdown of the ISO 42001 Certification Timeline by Phase The phases below overlap in practice. Treat the durations as effort estimates for a reasonably resourced program, not a strict sequence. Phase 1: Scoping and Gap Analysis (2–4 Weeks) Everything starts with two questions: which AI systems are in scope, and how far is your current governance from what the standard requires? The gap analysis maps your existing policies and controls against the standard’s clauses and Annex A controls, and produces the project plan for everything that follows. Get the scope wrong here and every later phase inherits the mistake. Phase 2: AIMS Design, Leadership, and AI Policy Development (2–4 Weeks) This phase establishes the skeleton of the management system: the AI policy, governance roles, objectives, and the leadership commitments the standard requires. Executive sign-off is the gating item. The documents are not hard to write. Getting senior leadership to formally own AI governance is where programs stall. Phase 3: AI Risk and Impact Assessments (2–6 Weeks) ISO 42001 requires both AI risk assessments and AI impact assessments, and the distinction matters. Risk assessments look at what could go wrong for the organization. Impact assessments look at consequences for individuals and society, which is a newer discipline for most teams. This phase takes longer when you have many AI systems, high-risk use cases, or no prior methodology to adapt. The output feeds directly into your Statement of Applicability (SoA), the document that maps which Annex A controls you have selected and why. Insider Note: Impact assessments are where auditors probe hardest, because they are the most distinctive part of ISO 42001 compared with ISO 27001. A recycled security risk register with “AI” pasted into it will get picked apart in Stage 2. Build the impact assessment methodology properly the first time. Phase 4: Controls Implementation (2–10 Weeks) The longest phase. Here you implement the Annex A controls selected in your SoA: AI system lifecycle documentation, data governance for training data, human oversight mechanisms, transparency measures, supplier management for third-party AI, and so on. Duration depends almost entirely on the gap analysis results. Organizations with mature engineering practices often find they already do much of this and just need to document it. Organizations without formal AI development processes are building from zero. Phase 5: Documentation, Training, and Evidence Collection (2–8 Weeks) Certification requires proof that the system operates, not just that it exists on paper. That means records: training completion logs, risk assessment outputs, review meeting minutes, monitoring reports. This phase runs partly in parallel with implementation, but it cannot be compressed below a certain floor because auditors want to see evidence generated over time, not a folder of documents all created the week before Stage 1. Phase 6: Internal Audit and Management Review (2–4 Weeks) The standard requires an internal audit of the AIMS and a formal management review before the certification audit. This is your dress rehearsal. A good internal audit surfaces nonconformities while they are still cheap to fix. Skipping or rushing it is a false economy that shows up later as Stage 2 findings. Phase 7: Stage 1 Certification Audit (1–2 Weeks) The certification body reviews your documentation and assesses readiness for Stage 2. The audit itself takes 1 to 3 days for most organizations. The auditor examines your scope statement, AI policy, risk and impact assessment methodology, SoA, and internal audit results, then issues findings. The 1–2 week window covers the audit plus the report. Phase 8: Closing Nonconformities (2–4 Weeks) Almost every Stage 1 produces findings.
CMMC requirements started appearing in Department of Defense contracts on November 10, 2025, when the final DFARS rule took effect. By November 10, 2028, the clause at DFARS 252.204-7021 must appear in every solicitation and contract where contractor systems process, store, or transmit Controlled Unclassified Information (CUI). For most of the Defense Industrial Base (DIB), the math is blunt: pass a CMMC assessment or lose eligibility for DoD work. A CMMC readiness assessment is how you find out whether you’d pass before the stakes are real. It’s a structured review of your environment, documentation, and evidence against the requirements of the Cybersecurity Maturity Model Certification, done before you sit for a self-assessment or a Certified Third-Party Assessment Organization (C3PAO) audit. A good one tells you exactly where you stand and what to fix first. This guide covers what a readiness assessment includes, how the process works at each CMMC level, what it costs, how long it takes, and how to pick someone to run one. What Is a CMMC Readiness Assessment? A CMMC readiness assessment is a pre-certification evaluation that measures your organization against the specific requirements of your target CMMC level. It examines your scope, implemented controls, System Security Plan (SSP), Plan of Action and Milestones (POA&M), and the evidence supporting them, then produces a gap analysis and a remediation roadmap. The purpose is simple: surface every deficiency while it’s still cheap to fix. An assessor who finds a scoping error during a readiness review costs you a few weeks of rework. A C3PAO who finds the same error during a certification assessment can cost you the assessment fee, months of delay, and in some cases contract eligibility. How It Differs From an Official C3PAO Audit An official CMMC Level 2 certification assessment is conducted by a C3PAO accredited by the Cyber AB, the official accreditation body for the CMMC ecosystem. The C3PAO’s findings are binding. Results go into the DoD’s assessment systems, and a passing result produces a CMMC status that contracting officers verify before award. A readiness assessment carries no official weight. Nothing gets filed or certified, and a poor result costs you nothing beyond the work needed to fix it. That’s the whole point. It’s the only stage in the entire process where failure is free. There’s also a conflict-of-interest rule worth knowing. A C3PAO cannot provide consulting and remediation services to an organization and then certify that same organization. If a C3PAO helps you prepare, a different C3PAO has to assess you. How It Differs From a Mock Assessment A mock assessment is a dress rehearsal. It simulates the certification assessment itself: assessors interview control owners, request evidence on the spot, and score findings the way a C3PAO would. A readiness assessment is broader and comes earlier, and its job is discovering and closing gaps rather than rehearsing the exam. Most organizations run a readiness assessment first, remediate, then run a mock assessment a few weeks before the real one to see whether staff and evidence hold up under live questioning. How It Differs From a Self-Assessment A self-assessment is a formal CMMC mechanism rather than a preparation exercise. CMMC Level 1 and a subset of Level 2 contracts let organizations self-assess, post the results to the Supplier Performance Risk System (SPRS), and have a senior official affirm compliance annually. That affirmation is a representation to the government, and false or careless affirmations carry False Claims Act exposure. A readiness assessment is the check you run before making that representation, so the number you affirm reflects reality. Why a CMMC Readiness Assessment Matters Avoiding Failed Certification Attempts CMMC Level 2 covers all 110 security controls of NIST SP 800-171, evaluated against 320 assessment objectives. Every objective has to be met for a control to score, and there’s no partial credit. Organizations that skip readiness work routinely walk into certification believing they’re compliant because controls are “mostly” implemented. Mostly implemented scores the same as not implemented. Protecting DoD Contract Eligibility Under the phased rollout that began in November 2025, CMMC status is a condition of award. Prime contractors also have to flow the requirement down to subcontractors that handle Federal Contract Information (FCI) or CUI, and they’ve been pushing their supply chains hard. So a missed certification hurts twice: you lose the immediate contract, and you risk dropping out of a prime’s approved supplier pool during the exact window when those pools are being rebuilt around CMMC status. Reducing Remediation Costs and Delays Gaps found early get fixed on your schedule with your choice of solution. Gaps found during certification get fixed under deadline pressure, often with whatever expensive tooling can be deployed fastest. There’s a conditional CMMC status for organizations that pass with a limited POA&M, but closeout has to happen within 180 days, and only certain lower-weighted controls are POA&M-eligible in the first place. Readiness work keeps you out of that corner. Worth Knowing: The DoD Assessment Methodology The DoD Assessment Methodology weights each NIST SP 800-171 control at 1, 3, or 5 points, deducted from a starting score of 110. The floor is -203. To achieve even a conditional Level 2 status, you need a minimum score of 88. A handful of unmet 5-point controls, such as FIPS-validated encryption or multifactor authentication, can put certification out of reach on their own, so a readiness assessment should always show the point weight attached to every gap. When to Conduct a CMMC Readiness Assessment Before your first self-assessment. If a contract requires a Level 1 or Level 2 self-assessment, run readiness work before you post a score to SPRS. The score you affirm is a legal representation, and it’s far easier to fix the environment than to explain a misstated score later. When contract requirements are approaching. If CMMC language has shown up in a solicitation you plan to bid, or your prime has set a certification deadline, count backward. Remediation after a readiness assessment typically takes six to twelve months for organizations starting
CMMC certification costs between $4,000 and $30,000 at Level 1, $30,000 to $300,000 or more at Level 2, and $100,000 to well over $1 million at Level 3. Most contractors expect the audit fee to be the big number. It isn’t. The formal assessment typically accounts for only 25% to 40% of total spend, with preparation, remediation, and technology upgrades consuming the rest. The stakes changed in late 2025. The final 48 CFR acquisition rule took effect on November 10, 2025, which means CMMC requirements now appear directly in Department of Defense (DoD) solicitations and contracts. Starting in November 2026, Phase 2 of the rollout gives contracting officers the authority to require third-party certification for Level 2 work. If you handle Controlled Unclassified Information (CUI), certification is no longer optional, and the cost question becomes a budgeting exercise rather than a hypothetical. This guide breaks down every major cost category, what moves your number up or down, and how to keep the total under control. What Is CMMC Certification and Why Does Cost Vary? The Cybersecurity Maturity Model Certification (CMMC) is the DoD’s framework for verifying that companies in the Defense Industrial Base (DIB) actually protect the sensitive information they handle. The program, codified in 32 CFR Part 170, builds on the security requirements of NIST SP 800-171 and, at the top tier, selected controls from NIST SP 800-172. Costs vary so widely because you can’t buy CMMC off a shelf. Your environment has to reach a certain state and then stay there. A 15-person machine shop with one well-scoped CUI enclave faces a fundamentally different project than a 500-person prime contractor with CUI flowing through a dozen systems. Your starting security posture, the scope of your assessment boundary, and whether you build internally or hire help all move the total by six figures in either direction. Average CMMC Certification Cost at a Glance The DoD’s own published estimates are instructive. A triennial Level 2 certification assessment, including affirmations, is projected at roughly $105,000 for small entities and $118,000 for larger ones. Those figures cover only assessment and affirmation activities, though. The DoD excludes implementation costs from its estimates on the grounds that NIST SP 800-171 compliance has been contractually required under DFARS 252.204-7012 since 2017. Your real budget has to cover both. CMMC Certification Cost by Level CMMC Level 1 (Foundational) Cost: $5,000 – $30,000 Level 1 covers Federal Contract Information (FCI) and requires 15 basic safeguarding practices drawn from FAR 52.204-21. Because Level 1 permits an annual self-assessment with no third-party auditor, the costs are internal labor, basic tooling, and documentation. Small contractors with reasonable IT hygiene often land near the bottom of the range. The DoD estimates annual Level 1 assessment and affirmation activity at around $6,000 for a small entity, with the remainder of the range driven by any remediation needed to attest honestly. CMMC Level 2 (Advanced) Cost: $50,000 – $300,000+ Level 2 is where most of the DIB lands and where budgets get serious. It requires full implementation of all 110 security requirements in NIST SP 800-171, assessed across 320 individual objectives. For most contracts, a C3PAO (Certified Third-Party Assessor Organization) accredited by the Cyber AB has to conduct the assessment every three years. Market data puts C3PAO assessment fees at $30,000 to $100,000 depending on scope, site count, and complexity. Preparation dwarfs that figure for most organizations. Companies starting from a low maturity baseline routinely spend three to four times the assessment fee on readiness work before an auditor ever shows up. CMMC Level 3 (Expert) Cost: $300,000 – $1,000,000+ Level 3 adds 24 enhanced requirements from NIST SP 800-172 on top of a completed Level 2 certification, and the assessment is conducted by the government’s DIBCAC rather than a commercial C3PAO. DIBCAC charges no assessment fee, but don’t mistake free for cheap. The DoD estimated roughly $41,000 in additional implementation cost for the 800-172 controls alone, and total triennial assessment-related costs in the $146,000 to $159,000 range. Real-world totals run far higher once you account for the advanced tooling, threat hunting capability, and organizational changes Level 3 demands. Only contractors supporting the most sensitive programs need this tier. Worth Knowing: You can’t skip to Level 3. You can’t skip to Level 3. A final Level 2 certification with all POA&M items closed is a prerequisite for the same assessment scope, so Level 3 budgets always include a full Level 2 project first. CMMC Certification Cost Breakdown by Expense Category Gap Assessment and Readiness Planning Costs A gap assessment maps your current environment against NIST SP 800-171 and typically costs $1,500 to $20,000 depending on depth and scope. This is the most valuable dollar you’ll spend in the entire project, because everything downstream is priced off what it finds. Documentation and System Security Plan (SSP) Costs The System Security Plan (SSP) is the cornerstone document of any assessment, mapping every control to your specific implementation. Professionally developed SSPs and supporting policies run $12,000 to $60,000. A weak SSP is one of the most common reasons assessments stall or fail, so this is a poor place to economize. Remediation and Security Control Implementation Costs Closing the gaps is usually the largest line item: $20,000 to $150,000 or more. Multi-factor authentication, logging and SIEM deployment, encryption, access control restructuring, and incident response capability all live here. Organizations with mature security postures spend far less than those starting from scratch. Technology and Infrastructure Upgrade Costs Many contractors move CUI into a dedicated enclave rather than securing their entire network. Enclave platforms typically cost $300 to $400 per user per month. Others upgrade endpoint protection, replace unsupported systems, or migrate to government-grade cloud environments, each with its own licensing and migration costs. C3PAO Assessment and Audit Fees The formal Level 2 assessment runs $30,000 to $100,000, driven by assessor-days, number of sites, and evidence quality. Well-organized evidence directly reduces assessor time and therefore your invoice. Consulting and Advisory Fees Specialist consultants, including Registered Practitioners (RPs) and
After a SOC 2 and ISO 27001 engagement, there are two documents out of the whole pile that actually close deals: the SOC 2 attestation report and the ISO 27001 certificate. Everything else your engagement produces exists to create those two, support them, or keep them alive for another year. Companies routinely ask their auditor for a SOC 2 certificate, which doesn’t exist. They send a prospect their full ISMS documentation when a one-page certificate would have done. They pay for six months of readiness work and then can’t say what they’re holding at the end of it. So here’s the full list. What a SOC 2 engagement produces, what an ISO 27001 engagement produces, what a combined program produces, and who gets to see each one. Understanding SOC 2 and ISO 27001 Engagement Outputs The Core Difference: Report vs. Certificate SOC 2 is an attestation. A licensed CPA firm examines your controls against the Trust Services Criteria under standards set by the AICPA, then writes up what it found and signs an opinion. No certificate. No logo from the AICPA. No pass or fail stamp. What you get is the report, and it usually runs 60 to 120 pages. ISO 27001 is a certification. An accredited certification body audits your Information Security Management System (ISMS) against ISO/IEC 27001:2022, and if you conform, it issues a certificate of registration. The certificate itself is a page or two. All the detail lives behind it, in your ISMS documentation and the audit reports the certification body writes as it goes. SOC 2 Engagement Deliverables The SOC 2 Attestation Report The report is the engagement. The AICPA’s illustrative SOC 2 report lays out the standard structure: auditor’s report, management’s assertion, system description, the Trust Services Criteria in scope, and the controls tested with their results. A Type I covers control design at one point in time. A Type II covers whether those controls actually operated over a period, usually three to twelve months, and most enterprise buyers now won’t accept anything else. Independent Auditor’s Opinion Letter First section of the report, and the first thing anyone experienced turns to. It gives the scope, the examination period, and the auditor’s conclusion. An unqualified opinion means the description held up and the controls worked. A qualified opinion means the auditor found something material, and every serious reviewer will want to talk about it. Management Assertion Your leadership signs a written statement stating that the system description is accurate and that the controls were properly designed and are operating. It reads like a formality, and it isn’t. The auditor’s entire examination runs against what management asserts here, so overstating anything creates real exposure. System Description Usually the longest part of the report, and you write it, not the auditor. It covers the services in scope, your infrastructure, software, people, processes, how data moves, which subservice organizations you depend on, and the complementary user entity controls your customers have to run on their side for your controls to hold up. Trust Services Criteria Applied Security (the Common Criteria) is in every SOC 2. Availability, Processing Integrity, Confidentiality, and Privacy are optional, and the report names exactly which ones you picked. Whatever you decide during scoping ends up printed in a document your customers read for the next several years. Description of Tests of Controls and Results (Type II) The matrix: every control, what the auditor did to test it, and what came back, including exceptions. Reviewers spend most of their time here, because the exceptions tell them things the opinion letter won’t. Bridge Letter / Gap Letter Your report covers a fixed window, so one ending December 31 leaves a hole for a customer doing diligence in June. A bridge letter from your management, not the auditor, confirms that nothing material changed in the control environment between the report’s end date and today. You’ll write these often enough to keep a template. Management Letter and Observations Plenty of auditors also send an internal-only letter covering observations, minor exceptions, and suggestions that never reached the threshold of a qualified opinion. It’s the closest thing to free consulting you’ll get before next year’s audit starts. Insider Note: Ask early whether your auditor issues a management letter, and whether exceptions land in the report body or only in that letter. Firms handle this differently, and the answer decides what your customers see versus what stays behind your firewall. It rarely comes up in the proposal, but it changes how the finished report reads to a buyer. ISO 27001 Engagement Deliverables ISO 27001 Certificate of Registration The document everyone asks for. It names the certified legal entity, states the ISMS scope, identifies the certification body, carries an accreditation mark from a body recognized under the International Accreditation Forum such as UKAS or ANAB, and shows the validity dates. It’s good for three years as long as you pass annual surveillance audits. Read the scope statement carefully, on your own certificate as much as anyone else’s. A certificate covering one office or one product line says nothing about the rest of the business. Statement of Applicability (SoA) After the certificate, this is the document buyers request most. The Statement of Applicability runs through all 93 Annex A controls in ISO/IEC 27001:2022, says which apply to you, justifies the ones you excluded, and records where each stands. Auditors use it as the map of your control environment, and larger customers increasingly want to see it or a summary of it during diligence. Risk Assessment and Risk Treatment Plan Your methodology, the register it produced, and the Risk Treatment Plan showing what you decided to do about each significant risk: mitigate it with a control, transfer it, avoid it, or accept it. ISO 27001 is built around risk, so these documents are what justify every control decision recorded in the SoA. Information Security Management System (ISMS) Documentation The policy and procedure set, plus the operational records that prove any of it happens. Information
The EU AI Act’s transparency requirements take effect on 2 August 2026, and most of the companies they cover still think the rules are not their problem. Article 50 applies to any business that publishes AI-generated content or runs an AI system that talks to people in the EU. That includes the marketing team generating campaign images and the support team running a chatbot. It also covers the AI agents you’ve wired into customer email. Penalties reach €15 million or 3% of total worldwide annual turnover, whichever is higher, and you don’t need an office in Europe to be in scope. If your content or your chatbot reaches EU users, the obligations reach you. In a nutshell: if you publish AI-generated images or video, deploy chatbots or AI agents that interact with EU users, or publish AI-written text on matters of public interest, then yes, the EU AI Act applies, starting 2 August 2026. A quick word on the “AI Act delay” headlines. The Digital Omnibus package did push the high-risk system deadlines back, in some cases by more than a year, but it did not move the deployer obligations in Article 50. Companies that read those headlines and stood down their AI Act work made an expensive mistake, because the rules most likely to touch an ordinary business are the ones that stayed on the calendar. What Article 50 Actually Requires Article 50 of the AI Act sets out transparency obligations in four situations. In plain English: Tell people when they’re talking to AI. Systems designed to interact directly with people — chatbots, voice assistants, and AI agents — must make clear that the user is dealing with AI, unless that’s already obvious. Mark AI-generated content so machines can detect it. Providers of generative AI systems must mark outputs in a machine-readable format, typically through metadata and watermarking, so the content is detectable as artificially generated. Label deepfakes. Anyone deploying AI to generate or manipulate image, audio, or video content that resembles real people, places, objects, or events, and could falsely appear authentic, must disclose that the content is artificial. Label AI-generated text on matters of public interest. Text published to inform the public must carry a label if AI-generated or manipulated, unless a human reviewed it and a person or organization holds editorial responsibility for it. Article 50 also covers emotion recognition and biometric categorization systems, which carry their own disclosure duties. Far fewer businesses run into those, so this article sticks to the four above. The distinction running through all of this is provider vs deployer. The provider builds or supplies the AI system. The deployer uses it professionally. Most companies reading this are deployers. If You Use AI-Generated Images Realistic AI images sit closer to the deepfake rules than most marketing teams assume. The Act’s definition covers content depicting people, objects, places, and events that could falsely appear authentic to a viewer, which describes a large share of what image generators produce for campaigns, social posts, and landing pages. So what does “clearly and distinguishably labeled” mean? The threshold is best described by its failures: a tiny disclosure hidden in the website footer doesn’t qualify. Neither does a faint label on an image, a label that flashes for an instant in a video, or a disclosure buried in your terms and conditions. The label has to be visible right where someone sees the content, and it has to meet accessibility standards so people with disabilities can perceive it too. The Code of Practice proposes a standardized “AI” visual label, localized per language (“KI” in German, “IA” in French). It also draws a useful line between fully AI-generated content and AI-assisted content, with lighter requirements for the latter. A designer who used AI to extend a background is in a different position from a team publishing a fully synthetic image of a person who doesn’t exist. Important: The deepfake duty doesn’t care about intent. A flattering, harmless AI image of your CEO at an event that never happened is still a deepfake under the Act. Marketing teams generate this kind of content casually. From August, every one of those images needs a label. If You Deploy AI Agents or Chatbots The rule itself is simple: people must know they’re dealing with AI. The provider carries the design obligation, but as the deployer you’re the one putting the system in front of your customers, and you’re the one an EU regulator will contact if your branded assistant pretends to be human. The Act contains an exception for cases where it’s “obvious” the user is talking to AI, judged from the perspective of a reasonably well-informed and observant person. Don’t lean on it. What’s obvious to your product team isn’t obvious to every customer, and the human-sounding voice agents and email-writing AI agents rolling out right now are designed specifically to not feel like software. If an AI agent negotiates a renewal over email or handles a support ticket end to end, disclose it. Pro Tip: Put the Disclosure at the Start of the Interaction Put the disclosure at the start of the interaction, in the interface itself: “You’re chatting with an AI assistant.” A line in your privacy policy doesn’t meet the standard, and a disclosure that appears after the conversation ends is worthless. For voice agents, say it up front in the greeting. What Your AI Vendors Owe You The machine-readable marking obligation in Article 50(2) sits with providers — the companies supplying your generative AI tools. The final Code of Practice expects providers to apply at least two layers of marking where necessary, such as embedded metadata combined with watermarking, and to offer detection mechanisms so deployers, authorities, and researchers can verify whether a piece of content came from AI. One timing caveat: the Digital Omnibus gives generative AI systems already on the market before 2 August 2026 until 2 December 2026 to comply with the marking requirement. Every other Article 50 obligation stays on
Guides and Reports
AXIPRO STUDY New Study: Europe is hiring AI builders faster than AI governance professionals Axipro analyzed 3,519 AI-related job postings across eight EU countries. For every professional hired to keep AI lawful, safe and accountable, nearly seven were hired to build more of it, and the gap is widest exactly where you’d least expect. Take EU AI ACT READINESS QUIZZ 16 AI Builders : 1 AI Governors Sweden — Europe’s widest AI governance gap 3,519 Job Postings Analyzed 8 EU Countries 2 Role Categories: Builders vs Governors July 2026 Date of Job Postings Analyzed The findings Finding 1: Sweden hires 16 AI builders for every 1 person to govern them Throughout our data-set we found the same pattern across all eight countries: the more a nation hires to build AI, the less it hires to govern it. France runs eleven builders to every governor. Even Ireland, the most balanced in Europe, looks responsible mainly because the US tech giants headquartered there import global-governance discipline under overlapping DORA and AI Act pressure. 3.5→16 builders hired per governor, Europe’s most balanced country to its least. Ireland 3.5 Germany 5.7 Spain 6.0 Italy 7.1 Netherlands 7.2 Belgium 7.9 France 11.4 Sweden 16:1 0 4 8 12 16 Builders hired per AI governor Source: Axipro, 2026 Sweden has one of the strongest engineering cultures in Europe. It also carries the widest governance gap we measured: sixteen AI builders hired for every person hired to govern them. France sits close behind at eleven to one. The most balanced country, Ireland at 3.5 to one, looks responsible for a reason that has little to do with virtue. The US tech giants headquartered in Dublin import global governance discipline, and they do it under the combined weight of the AI Act and DORA, the EU financial-sector resilience regime in force since January 2025. Engineering strength does nothing to close a governance gap, and it may widen it. A country that ships AI faster produces more systems that fall under the Act’s scope and, on this evidence, fewer people positioned to document, monitor, and defend them. Being good at building AI offers no protection against governing it badly. The countries most confident in their technical talent are running the largest deficit against the law. Explore AI governance hiring by country Click any country to see how many AI builders it hires for every governance professional, and where it ranks against the rest of Europe. Germany — 5.7 builders per governorDE France — 11.4 builders per governorFR Spain — 6.0 builders per governorES Italy — 7.1 builders per governorIT Netherlands — 7.2 builders per governorNL Belgium — 7.9 builders per governorBE Ireland — 3.5 builders per governorIE Sweden — 16 builders per governorSE 3.5 — balanced 16 — widest gap Source: Axipro, 2026 Sweden 16builders for every governance professional Rank 1 of 8 · 20 governance roles vs 319 builder roles posted Only 30% of the AI governance roles name the AI Act Share this Embed this map Copy & paste — links back to Axipro Copy embed code Branded, one paste, backlink included. × Share this country insight Share this AI governance gap X / Twitter LinkedIn Facebook WhatsApp Bluesky Email Copy link Choose a platform or copy the link. A view of the same country-level dataset behind the interactive map: governance roles, builder roles, builder-to-governance ratio, and the share of governance postings that name the EU AI Act. AI governance jobs Europe statistics by country: governance roles, builder roles, builder-to-governance ratio and AI Act mention percentage. Country Governance roles Builder roles Builder-to-governance ratio AI Act mention % Sweden 20 319 16.0:1 30.0% France 39 443 11.4:1 38.5% Belgium 38 299 7.9:1 39.5% Netherlands 61 439 7.2:1 31.1% Italy 40 284 7.1:1 45.0% Spain 64 384 6.0:1 28.1% Germany 88 501 5.7:1 27.3% Ireland 96 335 3.5:1 14.6% Source: Axipro analysis of AI builder, governance and compliance job postings across eight European countries. “AI Act mention %” is the share of governance postings that explicitly name the EU AI Act. Finding 2: The law nobody names. Most AI governance jobs still do not mention the EU AI Act Europe spent years drafting the AI Act. It cleared the European Parliament, survived the Digital Omnibus revisions, and now carries penalties that reach €35 million or 7% of global turnover for the most serious breaches, a ceiling that makes GDPR fines look modest. Yet fewer than three in ten of the governance roles created to handle it actually name the law in the job description. Among builder roles, the figure collapses to one in twenty-five. More than 7 in 10 Governance job descriptions do not mention the EU AI Act. This number rises to 9 in 10 for all AI job descriptions. Despite hiring for governance, risk, privacy, and compliance roles, most employers are not yet translating the EU AI Act into explicit job requirements. That disconnect should stop you. The people being hired to make Europe compliant are, for the most part, not being hired against the Act by name. They are titled around adjacent ideas: risk, ethics, model validation, data protection. Some of that work will map onto the Act’s requirements. Much of it will not, because a role written without the regulation in view rarely produces the conformity assessments, technical documentation, and human-oversight structures the Act specifically demands. Readiness is even thinner than the headcount suggests. Simply counting governance hires overstates how many people are actually working the law. What job descriptions actually name The EU AI Act is visible in governance roles — but still absent from most job ads. Across the laws and frameworks most relevant to AI governance hiring, the EU AI Act appears in fewer than three in ten governance postings, and only 4% of builder postings. Law or framework Governance roles naming it Builder roles naming it All roles naming it Governance mentions EU AI Act 28.5% 4.0% 7.6% 127 GDPR 26.9% 5.7% 9.6% 120 ISO 27001 11.4% 1.3% 2.8% 51
SOC 2 Hub
All you need to know about SOC 2 compliance
After a SOC 2 and ISO 27001 engagement, there are two documents out of the whole pile that actually close deals: the SOC 2 attestation report and the ISO 27001 certificate. Everything else your engagement produces exists to create those two, support them, or keep them alive for another year. Companies routinely ask their auditor for a SOC 2 certificate, which doesn’t exist. They send a prospect their full ISMS documentation when a one-page certificate would have done. They pay for six months of readiness work and then can’t say what they’re holding at the end of it. So here’s the full list. What a SOC 2 engagement produces, what an ISO 27001 engagement produces, what a combined program produces, and who gets to see each one. Understanding SOC 2 and ISO 27001 Engagement Outputs The Core Difference: Report vs. Certificate SOC 2 is an attestation. A licensed CPA firm examines your controls against the Trust Services Criteria under standards set by the AICPA, then writes up what it found and signs an opinion. No certificate. No logo from the AICPA. No pass or fail stamp. What you get is the report, and it usually runs 60 to 120 pages. ISO 27001 is a certification. An accredited certification body audits your Information Security Management System (ISMS) against ISO/IEC 27001:2022, and if you conform, it issues a certificate of registration. The certificate itself is a page or two. All the detail lives behind it, in your ISMS documentation and the audit reports the certification body writes as it goes. SOC 2 Engagement Deliverables The SOC 2 Attestation Report The report is the engagement. The AICPA’s illustrative SOC 2 report lays out the standard structure: auditor’s report, management’s assertion, system description, the Trust Services Criteria in scope, and the controls tested with their results. A Type I covers control design at one point in time. A Type II covers whether those controls actually operated over a period, usually three to twelve months, and most enterprise buyers now won’t accept anything else. Independent Auditor’s Opinion Letter First section of the report, and the first thing anyone experienced turns to. It gives the scope, the examination period, and the auditor’s conclusion. An unqualified opinion means the description held up and the controls worked. A qualified opinion means the auditor found something material, and every serious reviewer will want to talk about it. Management Assertion Your leadership signs a written statement stating that the system description is accurate and that the controls were properly designed and are operating. It reads like a formality, and it isn’t. The auditor’s entire examination runs against what management asserts here, so overstating anything creates real exposure. System Description Usually the longest part of the report, and you write it, not the auditor. It covers the services in scope, your infrastructure, software, people, processes, how data moves, which subservice organizations you depend on, and the complementary user entity controls your customers have to run on their side for your controls to hold up. Trust Services Criteria Applied Security (the Common Criteria) is in every SOC 2. Availability, Processing Integrity, Confidentiality, and Privacy are optional, and the report names exactly which ones you picked. Whatever you decide during scoping ends up printed in a document your customers read for the next several years. Description of Tests of Controls and Results (Type II) The matrix: every control, what the auditor did to test it, and what came back, including exceptions. Reviewers spend most of their time here, because the exceptions tell them things the opinion letter won’t. Bridge Letter / Gap Letter Your report covers a fixed window, so one ending December 31 leaves a hole for a customer doing diligence in June. A bridge letter from your management, not the auditor, confirms that nothing material changed in the control environment between the report’s end date and today. You’ll write these often enough to keep a template. Management Letter and Observations Plenty of auditors also send an internal-only letter covering observations, minor exceptions, and suggestions that never reached the threshold of a qualified opinion. It’s the closest thing to free consulting you’ll get before next year’s audit starts. Insider Note: Ask early whether your auditor issues a management letter, and whether exceptions land in the report body or only in that letter. Firms handle this differently, and the answer decides what your customers see versus what stays behind your firewall. It rarely comes up in the proposal, but it changes how the finished report reads to a buyer. ISO 27001 Engagement Deliverables ISO 27001 Certificate of Registration The document everyone asks for. It names the certified legal entity, states the ISMS scope, identifies the certification body, carries an accreditation mark from a body recognized under the International Accreditation Forum such as UKAS or ANAB, and shows the validity dates. It’s good for three years as long as you pass annual surveillance audits. Read the scope statement carefully, on your own certificate as much as anyone else’s. A certificate covering one office or one product line says nothing about the rest of the business. Statement of Applicability (SoA) After the certificate, this is the document buyers request most. The Statement of Applicability runs through all 93 Annex A controls in ISO/IEC 27001:2022, says which apply to you, justifies the ones you excluded, and records where each stands. Auditors use it as the map of your control environment, and larger customers increasingly want to see it or a summary of it during diligence. Risk Assessment and Risk Treatment Plan Your methodology, the register it produced, and the Risk Treatment Plan showing what you decided to do about each significant risk: mitigate it with a control, transfer it, avoid it, or accept it. ISO 27001 is built around risk, so these documents are what justify every control decision recorded in the SoA. Information Security Management System (ISMS) Documentation The policy and procedure set, plus the operational records that prove any of it happens. Information

SOC 2 is not a certification, and no auditor will ever hand you a SOC 2 certificate. What you receive at the end of the audit is an attestation report: a detailed document, often 60 to 100 pages long, in which a licensed CPA firm expresses a professional opinion on your controls. That distinction sounds like pedantry until a prospect’s security team asks to see your “certificate” and you have nothing that looks like one. This article explains exactly what a SOC 2 report is, what it contains, how it differs from an ISO 27001 certificate, and how to talk about your SOC 2 status without misrepresenting it. Is SOC 2 a Certification or a Report? The Common Misconception About “SOC 2 Certification” Search volume tells the story: far more people look for “SOC 2 certification” than for “SOC 2 attestation,” and sales teams, procurement questionnaires, and even some auditors use the certification shorthand daily. The misconception is understandable. Every other major framework in the compliance stack, from ISO 27001 to PCI DSS, ends in something that looks like a pass. SOC 2 does not work that way, and treating it as if it does leads to awkward conversations during vendor due diligence. Why SOC 2 Is Technically an Attestation, Not a Certification A certification is a binary judgment issued by an accredited body: you meet the standard, or you do not. SOC 2 sits under the AICPA’s attestation standards, primarily SSAE 18 and its later amendments (SSAE 21 updated the relevant examination sections), specifically AT-C section 105 and AT-C section 205. Under those standards, an independent service auditor examines your controls and reports an opinion on them. Nobody “passes.” The auditor attests to what they found, in writing, with evidence. The output is a report, and the report is the entire deliverable. Understanding the SOC 2 Attestation Model What Is an Attestation Engagement? An attestation engagement is a formal examination in which a practitioner evaluates subject matter prepared by another party against defined criteria, then issues a written conclusion. In SOC 2, the subject matter is your system and its controls, the criteria are the AICPA’s Trust Services Criteria (Security, Availability, Processing Integrity, Confidentiality, and Privacy), and the party preparing the subject matter is you, the service organization. Security is the only mandatory category; the other four are scoped in based on your service commitments. The Role of the AICPA and Licensed CPA Firms The AICPA (American Institute of Certified Public Accountants) owns the SOC framework and the attestation standards behind it, but it does not perform audits and does not issue anything to your company. Only a licensed CPA firm can conduct a SOC 2 examination and sign the resulting opinion. That licensing requirement is the quality mechanism: the firm’s professional liability, independence rules, and peer review obligations stand behind the report. In practice, this means the assurance you get is only as strong as the auditor’s reputation and independence posture, which is why enterprise buyers often look at who signed the report almost as carefully as they look at what it says. How Attestation Differs from Certification and Accreditation The three terms describe different assurance models. Certification means an accredited certification body confirms conformity with a standard and issues a certificate, as happens with ISO 27001. Accreditation is one level up: it is the process by which national bodies, such as those coordinated through the International Accreditation Forum, authorize those certification bodies to certify in the first place. Attestation involves no certificate and no accreditation chain. A CPA firm examines evidence and expresses an opinion under professional standards. The credibility comes from the auditor’s license and independence, not from a badge. What You Actually Receive After a SOC 2 Audit The SOC 2 Attestation Report Explained The deliverable is a confidential, restricted-use document addressed to your management and intended for your customers, their auditors, and other informed parties. It is dense by design. A prospect’s risk team reads it to understand what your system does, which controls you operate, how the auditor tested them, and what the auditor found. It replaces a certificate with something far more useful: evidence. Key Components of the Final Report Independent service auditor’s opinion. The first section, usually two to three pages, states the auditor’s formal conclusion on whether your system description is fairly presented and whether your controls were suitably designed (and, for Type 2, operating effectively). This is the section report readers check first. Management’s assertion. A signed statement in which your leadership formally asserts that the system description is accurate and that controls meet the applicable criteria. SSAE 18 made this management assertion a mandatory element, which means responsibility for the description sits with you, not the auditor. System description. The longest narrative section was prepared by management against the AICPA’s SOC 2 description criteria. It covers the services provided, infrastructure, software, people, data, processes, subservice organizations, and complementary user entity controls. Trust Services Criteria and controls tested. A mapping of each in-scope criterion to the specific controls you operate. This is where scoping decisions become visible: a report covering Security only looks very different from one covering all five categories. Results of testing. For Type 2 reports, a control-by-control table showing the tests the auditor performed and the results, including any exceptions. Sophisticated readers spend most of their time here, because exceptions and the auditor’s response to them reveal more than the opinion page does. What a SOC 2 Report Is NOT (No Certificate, No Logo, No Pass/Fail Badge) There is no official SOC 2 certificate, no numbered credential, and no register of “certified” companies you can be listed in. The AICPA licenses a standard SOC logo that service organizations may display for a limited time after report issuance, but the logo confirms only that an examination took place. It says nothing about the opinion inside. Anyone selling you a “SOC 2 certificate” as a standalone artifact is selling something the framework does not produce. Important: If
Most teams walk into a SOC 2 audit expecting standard requirements for their password policy: minimum length, 90-day rotation, one uppercase letter, one symbol, and so on. But there is no such checklist. The AICPA never published a list of mandatory password rules, and the federal guidance that most auditors lean on has thrown out half of what passed for best practice a decade ago. Beyond compliance, this is remains a crucial cybersecurity control: Stolen and brute-forced credentials still drive a large share of breaches, and password policies are the main way to mitigate this risk. This guide covers what SOC 2 expects around passwords, where those expectations come from, and how to build a policy that satisfies an auditor without making your security worse. What Are SOC 2 Password Requirements? SOC 2 password requirements are the access controls that a service organization implements to govern how passwords are created, stored, enforced, and retired, all in service of the Trust Services Criteria. The important word is controls, not rules. SOC 2 does not hand you a specification. It asks whether your controls are suitably designed and operating effectively to keep unauthorized people out of your systems. The Role of Passwords in the SOC 2 Trust Services Criteria The Trust Services Criteria, developed by the AICPA, are the evaluation standard for every SOC 2 report. Passwords sit inside the Security category, which is mandatory in all SOC 2 engagements, and specifically inside the Common Criteria series CC6, covering logical and physical access. Passwords are one of the most basic logical access controls you have, and one of the most scrutinized, because CC6 is usually the most evidence-intensive part of the entire audit. Relevant Common Criteria: CC6.1, CC6.2, and CC6.3 CC6.1 covers the controls that restrict logical access to systems, infrastructure, and data, this is where your password policy, MFA enforcement, and account lockout settings live. CC6.2 governs how access is granted, modified, and removed, meaning your provisioning workflows, access reviews, and offboarding processes are all evaluated here. CC6.3 focuses on the removal of access when it is no longer needed and the management of privileged credentials specifically. Together, these three criteria map to the full lifecycle of a credential: creation, ongoing use, and retirement. An auditor working through CC6 will expect evidence at every stage. Does SOC 2 Mandate Specific Password Rules? No. The AICPA is explicit that the Trust Services Criteria do not define the controls an organization must have. You identify and implement controls that meet the criteria, and the auditor evaluates them. That means there is no AICPA-mandated minimum length, no required rotation interval, and no prescribed complexity formula. What the auditor checks is whether your stated controls exist, work, and reasonably prevent unauthorized access. Insider note: Auditors rarely fail you for choosing a 10-character minimum over 12. They fail you when your written policy says one thing and your actual system configuration says another. Consistency between the policy document and the enforced setting matters far more than the specific number. Why Password Requirements Matter for SOC 2 Compliance Preventing Unauthorized Access Credentials are the front door. The 2025 Verizon DBIR found that stolen credentials remained the single most common initial access vector, appearing in 22% of breaches, and that brute force attacks against basic web applications nearly tripled year over year. Strong authentication controls are the difference between an attacker hitting a wall and an attacker walking straight in with a valid login. Reducing Data Breach Risk Weak or reused passwords feed credential stuffing, where attackers replay username and password pairs harvested from earlier breaches against your login pages. Reuse is rampant: research from Microsoft’s Digital Defense Report routinely finds that the majority of people reuse passwords across services. A single leaked password elsewhere becomes a working key to your environment unless your controls catch it. Demonstrating Logical Access Controls to Auditors SOC 2 is an attestation. It is not enough to be secure; you have to prove it with evidence. Well-designed password controls produce exactly the artifacts an auditor wants: configuration screenshots, enforcement logs, MFA reports, and access review records. Good controls and good evidence are two sides of the same coin, and an internal audit process that routinely collects this evidence makes the formal engagement significantly less stressful. Core SOC 2 Password Requirements Although SOC 2 prescribes nothing specific, a defensible password policy almost always addresses the same set of controls. These are what auditors expect to see and what your peers in compliance treat as table stakes. Minimum Password Length Length is the strongest single lever for password entropy, and modern guidance favors it over everything else. A common defensible baseline is at least 12 characters for standard user accounts, with longer requirements for service and admin accounts. NIST SP 800-63B recommends that verifiers support passwords up to 64 characters so that passphrases and password-manager output are never truncated, an important implementation detail that many teams overlook. Password Complexity and Blocklists Old-style complexity rules, one uppercase, one symbol, one number, are fading, and for good reason. They push users toward predictable substitutions without meaningfully raising entropy. The more effective control is a blocklist: screening new passwords against dictionaries of common and previously breached credentials and rejecting matches. Tools like Have I Been Pwned’s Pwned Passwords API make this straightforward to implement. This stops Password1! from sneaking through even though it technically satisfies a legacy complexity rule. Password Rotation and History Forced periodic rotation is the control most teams keep out of habit, and it is also the one that modern guidance most clearly discourages. Rotation pushes users toward predictable patterns, Spring2025 becoming Summer2025, without improving security in any measurable way. Password history settings, which prevent the immediate reuse of recent passwords, still have a place, but blind calendar-based expiry should be replaced with event-driven resets: force a change when there is evidence of compromise, not because the calendar says 90 days have passed. Account Lockout After Failed Login Attempts An account

The identity and access management market will pass $25 billion in 2026, and it is crowded with vendors that all make the same promise: the right people get the right access to the right resources at the right time. The hard part of any IAM solutions comparison is not finding capable products. It is that the leading platforms were each built to solve a different problem first, then expanded outward. Okta started with access. SailPoint started with governance. CyberArk started with privilege. Choose by brand reputation alone, and you risk buying a governance tool to solve an access problem, or paying enterprise prices for capabilities a mid-market team will never switch on. This guide compares the major providers by what they are actually good at, then walks through how to match one to your environment. What Is an IAM Solution? An IAM solution is the set of technologies that manages digital identities and controls what each identity can access. NIST frames the goal simply: ensure the right people and things have the right access to the right resources at the right time. In practice, that breaks into a few core functions: authenticating users (proving they are who they claim), authorizing them (deciding what they may do), and administering the account lifecycle as people join, move, and leave. The category splits into recognizable disciplines. Access management (AM) handles authentication and single sign-on. Identity governance and administration (IGA) handles who should have access and proves it to auditors. Privileged access management (PAM) protects the high-value accounts that can change infrastructure or read sensitive data. Most vendors now sell across these lines, but few are equally strong in all of them. That gap is the whole reason a comparison is worth doing. Why Comparing IAM Solutions Matters in 2026 Identity is now the primary attack surface. Stolen credentials and phishing remain among the top routes attackers use to get inside, which is why identity spending keeps climbing even when other security budgets flatten. The IAM market reached roughly $22 billion in 2025 and is on track for about $25 billion in 2026, growing near 15 percent a year, according to Fortune Business Insights. Two shifts make the comparison harder than it was a few years ago. First, the workforce went hybrid and cloud-first, so identity has to span on-prem systems, SaaS, and multi-cloud at once. Second, machine identities exploded. Your choice of platform now locks in how well you can govern not just employees but the service accounts, tokens, and AI agents multiplying across your environment. Gartner has reported that roughly 48 percent of organizations still lack a written IAM strategy — a serious problem, because a comparison is worth little if it is not anchored to documented requirements. Vendor demos are designed to make every product look like the obvious answer. Key Criteria for Comparing IAM Solutions A useful comparison rests on a consistent scorecard rather than the feature checklists vendors supply. The criteria below are the ones that tend to decide satisfaction two years after purchase. Core Identity and Access Capabilities Start with the fundamentals: single sign-on, multi-factor authentication, lifecycle provisioning and deprovisioning, and access certification. The differentiator in 2026 is adaptive, risk-based authentication that weighs device, location, and behavior before granting access, alongside phishing-resistant methods such as passkeys. A tool that only does password-plus-OTP is already behind. Deployment Options: Cloud-Native, Hybrid, and On-Premises Deployment model shapes cost, speed, and control. Cloud-native SaaS platforms deploy fastest and shift maintenance to the vendor. On-prem suits organizations with strict data-residency rules or deep legacy systems. Hybrid is the common reality, and the question to ask is how gracefully a platform bridges old and new — not whether it claims to. Integration Capabilities with Existing Infrastructure An IAM platform is only as good as its connectors. Look for prebuilt integrations with your core systems, directory services, HR platforms, and major SaaS apps, plus open standards support: SAML, OIDC, SCIM, and increasingly standards for continuous authorization. A thin connector catalog means custom engineering, which is where budgets quietly disappear. Scalability for Enterprise vs. Mid-Market Organizations Scale is not only user count. It is the number of applications, directories, and identity types a platform can govern without performance or administrative strain. Enterprise suites assume a dedicated identity team. Mid-market tools assume a stretched IT generalist. Buying the wrong tier means either paying for unused complexity or hitting a ceiling within two years. Pricing Models and Total Cost of Ownership Headline per-user pricing rarely reflects real cost. Implementation, professional services, connector licensing, premium support, and the internal staff time to run the platform often exceed the subscription itself. Compliance and Audit Support For regulated industries, audit support is a core feature, not a bonus. Strong platforms run access certification campaigns, segregation-of-duties checks, and audit-ready reports aligned with frameworks such as SOX, HIPAA, ISO 27001, and PCI DSS. The NIST Digital Identity Guidelines (SP 800-63, revised in 2025) are a useful reference for the assurance levels your authentication should meet. Vendor Support, Stability, and Roadmap You are buying a multi-year relationship. Financial stability, support quality, and a credible roadmap matter as much as today’s feature set, especially as the market consolidates and converges. A vendor that gets acquired or pivots can leave you maintaining a product on a slow decline. Pro Tip: Comparing Quotes When you compare quotes, normalize them to a three-year total cost of ownership that includes implementation and at least one major version upgrade. Vendors that look cheap per seat sometimes carry the heaviest services bill, and the gap usually shows up in year one, not at signing. IAM Solutions Compared: The Leading Providers The vendors below dominate enterprise shortlists. Each entry notes the problem the platform solves best — which is the most reliable way to read past the marketing. Okta Workforce Identity Cloud Okta is the largest independent identity vendor and was named a Leader in the 2025 Gartner Magic Quadrant for Access Management for the ninth straight year. Its strength is breadth of
Researchers who buy second-hand drives off online marketplaces keep finding the same thing: live data. A widely cited study by Blancco Technology Group found that 42% of used drives sold on eBay still held recoverable information, including financial records and personal data the previous owners assumed was long gone. The drives were not hacked; they were thrown away by organizations that treated deleting a file as the same thing as destroying it. Secure data disposal is where many compliance programs fail. ISO 27001, SOC 2, and GDPR all demand it, but they describe it in different languages, enforce it through different mechanisms, and punish failure in very different ways. This article sets out what each framework requires, where the requirements overlap, and how to run a single disposal program that satisfies all three at once. Why Secure Data Disposal Matters Across Compliance Frameworks Disposal is the last link in the data lifecycle, and the easiest one to skip. An organization can run flawless access controls, encryption, and monitoring for years and still cause a reportable breach the moment one unwiped laptop leaves the building. A recoverable drive in a recycling skip is functionally identical to an open database on the internet, and auditors and regulators know it. Most disposal failures are unforced errors: a control that was already written into policy but never carried through to the actual hardware. The gap between having a disposal policy and proving this specific drive was destroyed is exactly where audits and breach investigations live. Defining Secure Data Disposal: Key Terms and Concepts What Is Secure Data Disposal? Secure data disposal is the end-to-end process of removing data and the equipment that holds it from active use, in a way that prevents its recovery. It covers the full lifecycle end: deletion of data while a system is still live, sanitisation of media that will be reused, physical destruction of media that will not, and the safe handling of equipment that is recycled, returned to a lessor, or sold. Disposal is the goal. The methods are how you get there. What Is Secure Data Destruction? Secure data destruction is the subset of disposal that renders media permanently unusable or its contents mathematically irretrievable. Shredding a drive, pulverising it, incinerating it, or destroying the encryption keys that make an encrypted disk readable are all forms of destruction. Destruction is one route to disposal, and it is the right route when the data is highly sensitive, or the media will never be reused. Secure Data Disposal vs. Secure Data Destruction: What Is the Difference? The distinction matters more than it looks. Disposal is the outcome you owe to every framework: data gone, unrecoverable, equipment handled appropriately. Destruction is just one of the methods. You can dispose of data without destroying the hardware by sanitising a drive thoroughly enough to reuse it. Confusing the two leads to two classic mistakes: destroying assets that could have been securely wiped and reused, and assuming a quick deletion counts as disposal when it does not. Important: Emptying the recycle bin, formatting a drive, or hitting delete does not dispose of data under any of these frameworks. Standard deletion only removes the pointer to the data; the bits remain until they are overwritten. Every framework discussed here expects the data to be unrecoverable, which is a far higher bar than not visible. What ISO 27001 Requires for Secure Data Disposal ISO/IEC 27001 handles disposal through a small cluster of Annex A controls that auditors read as a single process rather than in isolation. The two controls that do most of the work are 7.14 and 8.10. For a deeper look at how these controls fit into a broader compliance program, see our ISO 27001 implementation guide. ISO 27001 Annex A 7.14: Secure Disposal or Re-Use of Equipment Annex A 7.14 is a physical control. Before any equipment is disposed of or reused, the organisation must check whether it holds information assets or licensed software and ensure those are permanently erased or the media physically destroyed. It applies to servers, laptops, desktops, mobile devices, printers, network gear, and any storage media: if it ever processed information, it is in scope. The control replaces the older 2013 clause 11.2.7 and adds explicit expectations around removing identifying markings and handling end-of-occupancy scenarios. ISO 27001 Control 8.10: Information Deletion Annex A 8.10 is a technological control, and it focuses on the data rather than the box. It requires information stored in systems, devices, or media to be deleted when it is no longer required, and rendered unrecoverable. The cleanest way to keep these straight: 8.10 governs the data while it is in use or reaches its retention limit; 7.14 governs the hardware at end of life. Most retention-driven deletion sits under 8.10; most decommissioning sits under 7.14. ISO 27001 Control 8.12: Data Leakage Prevention and Its Role in Disposal Control 8.12 is rarely filed under disposal, but improperly discarded media is one of the oldest data leakage channels there is. A drive that leaves your control with recoverable data on it is a leak, regardless of how it left. Treating disposal as part of your leakage prevention posture forces the right question at the right time: what could walk out the door on this device, and has it actually been removed? Physical Destruction and Irretrievable Erasure Under ISO 27001 ISO 27001 offers two broad routes: physically destroy media that holds information, or erase and overwrite it so retrieval by a malicious party is precluded. The standard cross-references ISO/IEC 27040 for detailed sanitisation methods. The unifying requirement is that recovery should be impractical, not merely inconvenient. Deletion alone never satisfies this. Overwriting, Full-Disk Encryption, and Other Approved Methods Overwriting user-accessible storage with multiple passes is acceptable for many sensitivity levels. Full-disk encryption changes the economics of disposal entirely: if a device is encrypted from day one and the keys are properly managed, secure disposal can be as simple as destroying the keys, a technique known as

A business continuity plan that has never been tested is, to a SOC 2 auditor, a document and nothing more. The Availability criteria do not award credit for a polished plan sitting in a shared drive. They ask for evidence that you ran the plan, watched it work or fail, recorded what happened, and fixed what broke. That gap — between having a plan and proving it works — is where most availability findings originate. Business continuity plan testing for SOC 2 is the exercise that turns your plan into auditable evidence. It maps directly to Availability criterion A1.3, one of the few SOC 2 controls that explicitly requires you to test something rather than merely document it. This guide covers what counts as a valid test, the test types auditors accept, a step-by-step process, the exact evidence you need, and the mistakes that turn a routine review into a finding. What Is Business Continuity Plan Testing in the Context of SOC 2? Business continuity plan (BCP) testing is the structured validation of whether your organization can keep critical operations running — and restore them within defined targets — during a disruption. In a SOC 2 context, the testing is not freeform. It must produce dated, traceable evidence that the recovery procedures in your plan actually work, that the people involved know their roles, and that systems and data come back within your stated recovery objectives. Why SOC 2 Requires Business Continuity Plan Testing SOC 2 is an attestation against the AICPA’s Trust Services Criteria, and the Availability category exists specifically for organizations that make uptime or resilience commitments to customers. A plan you never exercise cannot demonstrate operating effectiveness over the audit period — which is the entire point of a Type 2 examination. Testing is the control that converts a static plan into a recurring, observable activity an auditor can sample. SOC 2 Trust Services Criteria and BCP Testing Requirements Availability is one of the five Trust Services Criteria, and it is optional, included only when your service commitments warrant it. When in scope, it is built around three sub-criteria: A1.1 addresses capacity management. A1.2 addresses recovery infrastructure and backup processes. A1.3 addresses the testing of recovery procedures. BCP testing lives squarely in A1.3, with A1.2 supplying the backups and infrastructure that the test validates. Availability Criteria A1.2 and A1.3 Explained Per the AICPA’s Trust Services Criteria, A1.2 requires the entity to design, implement, operate, and monitor environmental protections, recovery infrastructure, and data backup processes that meet its availability objectives. In plain terms: you need real backups, stored away from production, with recovery infrastructure ready to use. A1.3 then requires the entity to test recovery plan procedures supporting system recovery to meet its objectives. The two work as a pair: A1.2 builds the capability, A1.3 proves it functions. Important: The most common A1.3 gap is not a missing test. It is a test that never validated the recovery objectives. Teams run a tabletop, write “no issues found,” and move on — but the plan claims a 4-hour RTO that no one ever measured against an actual restore. If your plan states recovery targets, your test evidence must show whether you met them. A test that does not measure against your RTO and RPO leaves the most important question unanswered. What Auditors Look for During a BCP Test Review Auditors want proof that the test happened, proof that it was meaningful, and proof that it led somewhere. Concretely, that means a test plan with a defined scenario, a dated record of execution with participants, results measured against your recovery objectives, a list of gaps or issues found, and evidence that those issues were remediated. A test that finds nothing and changes nothing is treated with suspicion — because real tests almost always surface something. Types of Business Continuity Plan Tests Accepted for SOC 2 SOC 2 does not mandate a specific test type. It expects the rigor of the test to match the criticality of what you are protecting. The four common approaches sit on a spectrum from low-effort, low-disruption to high-effort, high-assurance. Tabletop Exercises A tabletop exercise is a facilitated discussion where key personnel talk through a disruption scenario and their responses. It is cheap, fast, and excellent for confirming that people understand their roles and that the plan reads coherently. Its limit is obvious: nobody actually recovers anything. For many organizations a tabletop is a legitimate annual test, especially in the first audit cycle, but auditors expect more rigor as a program matures. Walkthrough and Simulation Tests A simulation applies a specific scenario and asks the team to perform recovery actions, not just describe them. It is more involved than a tabletop and far better at exposing the gaps that only appear when people touch the tools. Simulations are where teams discover that a runbook references a system that was decommissioned, or that the on-call engineer lacks the access the plan assumes. Full Interruption Tests A full interruption test shuts down primary systems and shifts operations entirely to the recovery environment. It is the most comprehensive validation available and the only one that proves your failover genuinely works end to end. It also carries real operational risk, so it demands thorough planning and is usually reserved for mature programs and the most critical systems. Parallel Testing Parallel testing activates recovery systems alongside production without taking the primary offline, then compares the two to confirm the recovery environment performs as expected. It delivers much of the assurance of a full interruption test while sparing the business the disruption. For most SaaS and cloud-hosted services, parallel testing of failover and restore is the sweet spot between confidence and risk. How to Test Your Business Continuity Plan for SOC 2 Compliance The sequence below aligns with the contingency planning process in NIST’s Contingency Planning Guide, SP 800-34, which auditors widely treat as authoritative for resilience practices. Each step produces an artifact, and the artifacts together form

A SOC 2 auditor will not ask whether you have an incident reporting policy. They will ask you to pull a specific incident from the last twelve months and walk them through it: when it was detected, who classified it, when it was escalated, who was notified, and how it was closed. The policy is the easy part. The part that fails audits is the gap between what the document says and what the timestamps actually show. Incident reporting sits at the center of the SOC 2 System Operations criteria, and it is one of the most frequently exception-flagged areas in Type 2 reports. The reason is consistent: teams treat reporting as paperwork generated after the fire is out, rather than as a controlled process that produces evidence at every step. This guide breaks down how to build a reporting process that an auditor can test, sample, and sign off on without a finding. What Is the Incident Reporting Process in SOC 2? The incident reporting process is the documented, repeatable sequence your organization follows from the moment a security event is detected to the moment the incident is formally closed and archived. It governs how events are logged, classified, escalated, communicated, and recorded. Reporting is not a single notification email. It is the connective tissue that links detection, response, and post-incident review into an auditable chain. How SOC 2 Defines a Security Incident SOC 2 does not hand you a rigid statutory definition. It works through the AICPA’s Trust Services Criteria, which frame an incident around a failure, or potential failure, of the system to meet the organization’s service commitments and security objectives. In practice, a security incident is any event that compromises, or could compromise, the confidentiality, integrity, or availability of systems or data. The criteria expect you to define this threshold yourself and apply it consistently, which is precisely what auditors test against. What Qualifies as a Reportable Security Incident Under SOC 2? An event becomes reportable when it crosses the threshold your own policy sets. The distinction matters. A blocked phishing email is a security event. A user who clicked the link and entered credentials is a reportable incident. SOC 2 rewards organizations that draw this line explicitly, because a clear definition is what makes consistent triage possible. Vague language like “significant events will be reported” invites the auditor to ask who decides what counts as significant, and on what basis. Examples of Security Incidents Relevant to SOC 2 Common reportable incidents include unauthorized access to production systems, credential compromise, malware or ransomware infection, data exfiltration or accidental disclosure, denial-of-service events affecting availability, lost or stolen devices holding company data, and misconfigurations that expose data to the public. Vendor and subprocessor breaches that touch your data belong on this list, too, since the criteria extend your responsibility into the supply chain. How Incident Severity Levels Are Established and Classified Severity classification drives everything downstream: how fast you respond, who gets pulled in, and which notification clocks start ticking. Most mature programs use a tiered scheme tied to business impact rather than technical noise. The point is not the labels you choose but the fact that the labels map to defined response times and escalation paths, and that the mapping is documented before an incident occurs, not invented during one. Auditors quietly judge your maturity by how few P1s you declare and how consistently you apply the tiers. A program that labels everything critical looks panicked; one that never escalates looks asleep. The strongest signal is a severity matrix with response-time SLAs next to each tier, and ticket history showing the tiers were actually applied as written. SOC 2 Incident Reporting Requirements There is no single “incident reporting requirement” in SOC 2. The obligation is distributed across several Common Criteria, and the auditor assembles a picture from all of them. Understanding which criteria govern reporting tells you exactly what evidence to keep. Which SOC 2 Trust Services Criteria Govern Incident Reporting? Incident reporting lives mainly in the CC7 (System Operations) series. CC7.2 covers monitoring system components to detect anomalies that may signal an incident. CC7.3 requires you to evaluate detected events to determine whether they are incidents and to take action. CC7.4 governs the response itself, including containment, eradication, and communication. CC7.5 addresses recovery and remediation. Communication obligations also reach into CC2.2 and CC2.3, which deal with internal and external information flow, and third-party incidents implicate CC9.2 on vendor risk. These are points of focus, not a checklist, but auditors use them to frame their testing. For a deeper look at how these criteria map to your broader compliance program, see our SOC 2 compliance guide. What Evidence Do Auditors Expect From Your Incident Reporting Process? Auditors want artifacts with time references, not assertions. That means incident tickets showing detection and closure timestamps, severity classifications with the name of who assigned them, escalation records, communication logs, and post-incident review notes. In a Type 2 examination they will trace one real incident end to end. Evidence pulled from a staging environment, or any artifact with no clear date, gets challenged immediately. Who Is Responsible for Reporting Security Incidents? Everyone reports; a defined role decides. SOC 2 expects that all staff know how to raise a suspected incident, and that a named function, often a security lead or incident commander, owns the determination of severity and the decision to escalate. The auditor will look for evidence that this ownership is real: a RACI chart is fine, but ticket history showing the right person actually classified and closed incidents is better. Step-by-Step SOC 2 Incident Reporting Process The following sequence maps cleanly to the lifecycle in NIST’s Computer Security Incident Handling Guide (SP 800-61), which auditors widely recognize as authoritative. NIST withdrew Revision 2 in April 2025 and released Revision 3, which reorganizes the lifecycle around the six functions of the Cybersecurity Framework 2.0. The underlying steps below remain the same; the framing simply shifts toward continuous risk management.

Most SOC 2 auditors will pick a handful of recent hires from your employee list and request one specific artifact: the completed background check, dated before the start date, sourced from a documented vendor. If you cannot produce it, that is an exception in your report. The control sits inside CC1.4, the Common Criteria provision the AICPA derives from COSO Principle 4, and it is one of the most reliably tested items in a first-year SOC 2 examination. Background screening is not the most technically complex part of SOC 2. It is, however, one of the most procedurally fragile. The policy looks simple on paper. Then a contractor starts a week early because someone needed help shipping a release, the vendor screening gets postponed, and a year later an auditor finds the gap in twenty minutes. This guide explains what SOC 2 actually requires when it comes to background checks, what auditors look for in practice, and how to build a screening programme that holds up under sampling. What Is a SOC 2 Background Check? A SOC 2 background check is the pre-employment screening a service organisation performs to verify that the people it hires can be trusted with access to systems and data inside the SOC 2 scope. It is the operational evidence that supports the abstract principle baked into the Trust Services Criteria: the organisation hires competent people of sound integrity, and it can prove it. In practice, that means a documented check performed by a third party that returns verified information about identity, criminal history, employment history, and, depending on the role, education and credit. The check is run against every new hire before they get logical or physical access to systems within scope. The result is stored, mapped to a named employee, and retrievable on demand. It is worth being clear on one thing: SOC 2 does not prescribe what a background check must contain. The AICPA criteria describe outcomes, not procedures. Your policy is what defines what gets checked, on whom, and how often. The auditor then tests whether you followed your own policy. Why SOC 2 Background Checks Are Important Insider risk is one of the few attack vectors that perimeter security cannot fix. An employee or contractor with legitimate credentials and undisclosed motives sits inside the network from day one. Background checks are how mature security programmes reduce the probability of that scenario before it begins. According to the Verizon 2024 Data Breach Investigations Report, insider threats continue to represent a persistent and costly category of security incidents, reinforcing why personnel vetting remains a foundational control. Auditors care for a related reason. The Control Environment criteria (CC1) sit at the top of the SOC 2 framework because everything else rests on the assumption that the people running the controls are competent and trustworthy. Skip the screening step, and the rest of the audit is built on a weaker foundation. That is why background check evidence is one of the first things auditors sample, and why a missing or late check shows up as an exception even when the rest of your control environment is strong. Insider Note: Auditors do not just check that the screening happened. They check the timing. A background check completed two months into employment is often treated the same as no check at all, because access to in-scope systems was granted before the control was operative. Time stamps matter as much as the document. SOC 2 Background Check Requirements Which Trust Service Criteria Require Background Checks? Background checks are explicitly referenced in the Common Criteria that apply to every SOC 2 engagement, regardless of which optional Trust Services Categories you include. The two controls that matter most are CC1.1 and CC1.4. CC1.1 establishes the entity’s commitment to integrity and ethical values. Background checks support this by demonstrating due diligence in selecting people who meet the organisation’s standards of conduct. CC1.4 is more direct: it derives from COSO Principle 4, which states that the entity demonstrates a commitment to attract, develop, and retain competent individuals in alignment with objectives. Within CC1.4, evaluating individual backgrounds is named as a specific point of focus. That is the hook auditors use. Because these are Common Criteria, they apply regardless of whether you are scoping Security only or adding Availability, Confidentiality, Processing Integrity, or Privacy. There is no version of SOC 2 that escapes them. Who Needs to Be Background Checked for SOC 2? The short answer: anyone whose role gives them logical or physical access to systems, data, or facilities within your SOC 2 scope. The longer answer requires you to draw the line in your own policy and stick to it. At a minimum, this includes full-time employees who join the organisation after the policy is in place. Most mature programmes extend the requirement to part-time employees, contractors who receive credentials, and outsourced personnel performing in-scope work. Vendors are usually handled differently — through contractual flow-down requirements rather than direct screening — but the principle is the same: people inside the trust boundary must be vetted. Roles with privileged access (engineers with production credentials, finance staff with payment system rights, support personnel handling customer data) often warrant deeper screening than baseline roles. Documenting this risk-based approach in your policy is good practice and helps you defend the design of your control during the audit. What Types of Checks Must Be Performed? The Trust Services Criteria do not specify which checks to run. That decision sits with the organisation, informed by role, jurisdiction, and regulatory context. A common baseline for SOC 2 purposes covers several distinct areas. Identity verification confirms the candidate is who they claim to be. Criminal history — national, state, or county-level depending on jurisdiction — flags relevant offences. Employment verification confirms the work history disclosed during hiring. Education verification matters for roles where credentials are material. For positions touching finance, payments, or fiduciary responsibility, a credit check may be appropriate. For roles with global reach, a global
ISO 27001 Hub
The latest resources and guides for ISO 27001 Certification
After a SOC 2 and ISO 27001 engagement, there are two documents out of the whole pile that actually close deals: the SOC 2 attestation report and the ISO 27001 certificate. Everything else your engagement produces exists to create those two, support them, or keep them alive for another year. Companies routinely ask their auditor for a SOC 2 certificate, which doesn’t exist. They send a prospect their full ISMS documentation when a one-page certificate would have done. They pay for six months of readiness work and then can’t say what they’re holding at the end of it. So here’s the full list. What a SOC 2 engagement produces, what an ISO 27001 engagement produces, what a combined program produces, and who gets to see each one. Understanding SOC 2 and ISO 27001 Engagement Outputs The Core Difference: Report vs. Certificate SOC 2 is an attestation. A licensed CPA firm examines your controls against the Trust Services Criteria under standards set by the AICPA, then writes up what it found and signs an opinion. No certificate. No logo from the AICPA. No pass or fail stamp. What you get is the report, and it usually runs 60 to 120 pages. ISO 27001 is a certification. An accredited certification body audits your Information Security Management System (ISMS) against ISO/IEC 27001:2022, and if you conform, it issues a certificate of registration. The certificate itself is a page or two. All the detail lives behind it, in your ISMS documentation and the audit reports the certification body writes as it goes. SOC 2 Engagement Deliverables The SOC 2 Attestation Report The report is the engagement. The AICPA’s illustrative SOC 2 report lays out the standard structure: auditor’s report, management’s assertion, system description, the Trust Services Criteria in scope, and the controls tested with their results. A Type I covers control design at one point in time. A Type II covers whether those controls actually operated over a period, usually three to twelve months, and most enterprise buyers now won’t accept anything else. Independent Auditor’s Opinion Letter First section of the report, and the first thing anyone experienced turns to. It gives the scope, the examination period, and the auditor’s conclusion. An unqualified opinion means the description held up and the controls worked. A qualified opinion means the auditor found something material, and every serious reviewer will want to talk about it. Management Assertion Your leadership signs a written statement stating that the system description is accurate and that the controls were properly designed and are operating. It reads like a formality, and it isn’t. The auditor’s entire examination runs against what management asserts here, so overstating anything creates real exposure. System Description Usually the longest part of the report, and you write it, not the auditor. It covers the services in scope, your infrastructure, software, people, processes, how data moves, which subservice organizations you depend on, and the complementary user entity controls your customers have to run on their side for your controls to hold up. Trust Services Criteria Applied Security (the Common Criteria) is in every SOC 2. Availability, Processing Integrity, Confidentiality, and Privacy are optional, and the report names exactly which ones you picked. Whatever you decide during scoping ends up printed in a document your customers read for the next several years. Description of Tests of Controls and Results (Type II) The matrix: every control, what the auditor did to test it, and what came back, including exceptions. Reviewers spend most of their time here, because the exceptions tell them things the opinion letter won’t. Bridge Letter / Gap Letter Your report covers a fixed window, so one ending December 31 leaves a hole for a customer doing diligence in June. A bridge letter from your management, not the auditor, confirms that nothing material changed in the control environment between the report’s end date and today. You’ll write these often enough to keep a template. Management Letter and Observations Plenty of auditors also send an internal-only letter covering observations, minor exceptions, and suggestions that never reached the threshold of a qualified opinion. It’s the closest thing to free consulting you’ll get before next year’s audit starts. Insider Note: Ask early whether your auditor issues a management letter, and whether exceptions land in the report body or only in that letter. Firms handle this differently, and the answer decides what your customers see versus what stays behind your firewall. It rarely comes up in the proposal, but it changes how the finished report reads to a buyer. ISO 27001 Engagement Deliverables ISO 27001 Certificate of Registration The document everyone asks for. It names the certified legal entity, states the ISMS scope, identifies the certification body, carries an accreditation mark from a body recognized under the International Accreditation Forum such as UKAS or ANAB, and shows the validity dates. It’s good for three years as long as you pass annual surveillance audits. Read the scope statement carefully, on your own certificate as much as anyone else’s. A certificate covering one office or one product line says nothing about the rest of the business. Statement of Applicability (SoA) After the certificate, this is the document buyers request most. The Statement of Applicability runs through all 93 Annex A controls in ISO/IEC 27001:2022, says which apply to you, justifies the ones you excluded, and records where each stands. Auditors use it as the map of your control environment, and larger customers increasingly want to see it or a summary of it during diligence. Risk Assessment and Risk Treatment Plan Your methodology, the register it produced, and the Risk Treatment Plan showing what you decided to do about each significant risk: mitigate it with a control, transfer it, avoid it, or accept it. ISO 27001 is built around risk, so these documents are what justify every control decision recorded in the SoA. Information Security Management System (ISMS) Documentation The policy and procedure set, plus the operational records that prove any of it happens. Information

Two controls decide whether your ISO 27001 business continuity plan survives an audit: Annex A 5.29 and Annex A 5.30. One keeps your security controls working while everything else is failing. The other gets your systems back online before the damage becomes permanent. Plenty of teams write a continuity policy that satisfies neither in the way a certification auditor expects, and they discover the gap during the Stage 2 audit, when it is expensive to fix. This article covers what ISO 27001:2022 actually requires for business continuity, the components an auditor will ask to see, the step-by-step build, and the mistakes that turn a continuity plan into a non-conformity. What Is an ISO 27001 Business Continuity Plan? An ISO 27001 business continuity plan is the documented set of procedures that keeps information security effective and critical ICT services available during a disruption. It is not a generic “keep the lights on” binder. Under ISO 27001, the plan protects the confidentiality, integrity, and availability of information when normal operations break down: a ransomware event, a cloud outage, a data center failure, or a supplier collapse. The plan lives inside your Information Security Management System (ISMS). It draws on your risk assessment, your asset register, and your Business Impact Analysis (BIA), and it feeds your disaster recovery procedures. Scope is the part people get wrong. ISO 27001 cares about the information security aspects of continuity, not every operational hiccup a full business continuity program might cover. Why You Need a Business Continuity Plan for ISO 27001 Compliance Downtime is expensive, and the bill arrives fast. For most organizations, the question is not whether a disruption will happen, but how quickly they recover when it does. There is also a hard compliance reason. You cannot certify to ISO 27001 while ignoring continuity. The standard requires you to maintain information security during disruption and to keep ICT able to support recovery, and an auditor will ask for the evidence. A continuity plan is where availability stops being a promise and becomes a tested capability. Let Axipro help you build a business continuity plan that’s practical, compliant, and audit-ready. Strengthen Your Business Continuity Strategy Schedule A Consultation ISO 27001 Requirements Related to Business Continuity Planning ISO/IEC 27001:2022 carries 93 Annex A controls across four categories: organizational, people, physical, and technological. Continuity sits in the organizational set, and two controls do the heavy lifting, supported by two more on the technical side. Annex A 5.29 – Information Security During Disruption A.5.29 requires you to maintain information security at an appropriate level when a disruption hits. The point is that security controls have a habit of degrading under pressure. People disable multi-factor authentication to “speed things up,” logging stops on a failover system, or access controls loosen while everyone scrambles. A.5.29 says the confidentiality and integrity of your information must be maintained even while availability is under threat. It is classed as both a preventive and a corrective control, meaning it should reduce the chance of an incident and also help resolve one already underway. Annex A 5.30 – ICT Readiness for Business Continuity A.5.30 is the technical engine. It requires that your ICT readiness is planned, implemented, maintained, and tested against business continuity objectives and ICT continuity requirements. In plain terms, your servers, networks, applications, and cloud services need a defined recovery path, each with a Recovery Time Objective (RTO) and Recovery Point Objective (RPO), and you need to prove the path works. This control is entirely new in the 2022 revision. It has no precedent in ISO 27001:2013, which is exactly why teams migrating from the older version so often have a gap here. Important: A.5.30 did not exist in ISO 27001:2013. If your continuity documentation was written against the old Annex A 17 cluster and never updated, you are missing a control the auditor will specifically test. Treat ICT readiness as a fresh requirement, not a relabel. Two technological controls back these up. Annex A 8.13 (Information Backup) requires backups to be taken and tested in line with an agreed policy, and Annex A 8.14 (Redundancy of Information Processing Facilities) covers the failover and redundancy that let critical systems keep running when a component dies. Relationship Between ISO 27001 and ISO 22301 This is where confusion is common. ISO 27001 requires the information security aspects of continuity. ISO 22301 is the dedicated standard for a full Business Continuity Management System (BCMS), covering people, facilities, supply chain, and operations far beyond information security. An ISO 27001 certificate does not certify your wider continuity program. The good news: both standards share the Annex SL high-level structure, so risk assessment, internal audit, management review, and document control carry across. Teams that already run ISO 27001 can layer ISO 22301 on top with far less effort than starting from scratch. Key Components of an ISO 27001 Business Continuity Plan Business Impact Analysis (BIA) The BIA is the foundation. It identifies your critical business processes, the ICT systems they depend on, and the cost of losing each one over time. It is where your recovery objectives come from, not from a vendor datasheet. A BIA also sets the Maximum Tolerable Period of Disruption (MTPD): the point beyond which an activity’s failure causes unacceptable damage. Risk and Disruption Scenario Assessment Your risk assessment identifies what could cause a disruption and how likely it is, feeding the Risk Treatment Plan and the Statement of Applicability (SoA) that records which controls apply. Continuity planning then runs concrete scenarios: ransomware, a regional outage, a key supplier failure, the loss of a data center. Response and Recovery Strategies For each critical system, you define how you will respond and recover: failover to a secondary site, restore from backup, or switch to a manual workaround. This links incident response to crisis management, the executive-level decision-making that kicks in when an incident escalates beyond a routine fix. Roles and Responsibilities Name real people, not departments. “IT will handle it” is the single most common

Most companies pursuing ISO 27001 certification cost analysis for the first time will spend between $10,000 and $50,000 in year one, and far less than half of that goes to the auditor. A 50-person SaaS company typically pays $10,000 to $22,000 in certification body fees alone, then doubles or triples that figure in implementation work, tooling, and internal hours before the Stage 2 audit even begins. The wide range exists because ISO 27001 certification cost is not a price tag; it is the sum of a dozen separate decisions: your scope, your security maturity, your certification body, and whether you build the ISMS yourself, hire a consultant, or run it through a compliance automation platform. This article breaks down every one of those costs, stage by stage and region by region, including the ones that never appear in vendor quotes. What Determines ISO 27001 Certification Cost? Six variables drive almost all of the variance between a $10,000 certification and a $150,000 one. Company Size and Employee Count Headcount is the single biggest cost driver because certification bodies calculate audit days (mandays) primarily based on the number of people working within the scope of your Information Security Management System (ISMS). The calculation is not arbitrary: accredited bodies follow the audit time tables in ISO/IEC 27006, which means a 20-person company and a 200-person company will receive structurally different quotes no matter how hard they negotiate. More employees also means more interviews, more evidence sampling, and more Annex A controls applied across more people. Scope and Complexity of the ISMS Scope is the variable you actually control. Your Statement of Scope defines which business units, systems, products, and locations fall inside the ISMS. A scope limited to one product line and the engineering team that runs it costs dramatically less to implement and audit than a whole-of-company scope. Complexity compounds this: bespoke infrastructure, regulated data types, and heavy third-party dependency chains all add controls, evidence, and audit time. Number of Physical and Cloud Locations Each physical site within scope can require its own audit visit, with travel costs on top. Multi-site organisations can reduce this through sampling (more on the square root rule later), but every additional location still adds something. Cloud environments count too: multiple cloud providers, regions, and tenancy models expand the technical scope auditors must cover, even when no travel is involved. Existing Security Maturity A company that already runs access reviews, maintains an asset inventory, and documents its incident response process is buying a much shorter journey than one starting from a blank page. The gap analysis exists precisely to price this difference. Organisations already aligned to SOC 2, NIST CSF, or Cyber Essentials Plus typically reuse 50 to 70 percent of their existing controls and evidence, which translates directly into lower implementation cost. Choice of Certification Body Certification bodies are not interchangeable on price. Large international names like BSI, Bureau Veritas, LRQA, and DNV charge premium day rates, often 30 to 50 percent above smaller accredited bodies, and their brand carries weight with enterprise procurement teams. What matters most is accreditation: a certificate issued by a body accredited by UKAS, ANAB, or another IAF (International Accreditation Forum) member carries international recognition. An unaccredited certificate is cheaper and close to worthless in serious sales conversations. Internal vs. External Implementation Approach The final driver is who does the work. Internal teams cost salary hours. Consultants cost fees. Platforms cost subscriptions. Each approach lands at a very different total, which is why this article dedicates a full section to it below. Average ISO 27001 Certification Cost Ranges The ranges below cover total first-year cost: implementation, tooling, and certification audits combined. They assume an accredited certification body and a sensibly defined scope. Cost for Small Businesses and Startups (1–50 Employees) A focused startup with a single product, cloud-native infrastructure, and a tight scope can realistically certify for $10,000 to $35,000 all-in. Lean implementations using templates or an automation platform sit at the bottom of that range. UK micro-businesses can find UKAS-accredited audit fees starting around £6,250, with day rates near £1,250. Cost for Mid-Sized Organizations (50–250 Employees) This is where most certifications happen, and where costs spread widest. Expect 8 to 12 initial audit days, $30,000 to $80,000 in total first-year spend, and a six to nine month timeline. Multiple departments, more mature customer requirements, and the first real multi-team coordination overhead all show up in the budget. Cost for Large Enterprises (250+ Employees) Enterprise certifications routinely exceed $100,000 in year one once you include program management, multiple sites, and large-scale audits. The audit fee alone can pass $50,000 for complex, multi-site scopes. At this scale, the internal time investment, covered under hidden costs below, often outweighs every external invoice. ISO 27001 Cost Breakdown by Stage Here is where the money actually goes, in roughly the order you will spend it. Cost of Purchasing the ISO 27001 Standard The official ISO/IEC 27001:2022 document costs CHF 155 (roughly $170) from the ISO store. Most teams also buy ISO 27002, the implementation guidance for the Annex A controls, for a similar amount. Budget $300 to $400 for both. Do not skip this purchase: implementing against second-hand summaries of the standard is a common source of audit findings. Gap Analysis Costs A consultant-led gap analysis before committing to anything else runs $2,000 to $10,000 depending on scope, while platform-based readiness assessments are often bundled into the subscription. The output, a clear map of where you stand against every clause and control, is what makes the rest of the budget predictable. ISMS Implementation Costs This is the largest and most variable line item: building the risk assessment, the risk treatment plan, the Statement of Applicability (SoA), and operationalizing the controls you have selected. Done internally, it consumes 200 to 600 hours of staff time over four to eight months. Done with consultants, expect $10,000 to $50,000 in fees for a typical SMB. Documentation and Policy Development Costs ISO 27001 requires a defined set of documented
Researchers who buy second-hand drives off online marketplaces keep finding the same thing: live data. A widely cited study by Blancco Technology Group found that 42% of used drives sold on eBay still held recoverable information, including financial records and personal data the previous owners assumed was long gone. The drives were not hacked; they were thrown away by organizations that treated deleting a file as the same thing as destroying it. Secure data disposal is where many compliance programs fail. ISO 27001, SOC 2, and GDPR all demand it, but they describe it in different languages, enforce it through different mechanisms, and punish failure in very different ways. This article sets out what each framework requires, where the requirements overlap, and how to run a single disposal program that satisfies all three at once. Why Secure Data Disposal Matters Across Compliance Frameworks Disposal is the last link in the data lifecycle, and the easiest one to skip. An organization can run flawless access controls, encryption, and monitoring for years and still cause a reportable breach the moment one unwiped laptop leaves the building. A recoverable drive in a recycling skip is functionally identical to an open database on the internet, and auditors and regulators know it. Most disposal failures are unforced errors: a control that was already written into policy but never carried through to the actual hardware. The gap between having a disposal policy and proving this specific drive was destroyed is exactly where audits and breach investigations live. Defining Secure Data Disposal: Key Terms and Concepts What Is Secure Data Disposal? Secure data disposal is the end-to-end process of removing data and the equipment that holds it from active use, in a way that prevents its recovery. It covers the full lifecycle end: deletion of data while a system is still live, sanitisation of media that will be reused, physical destruction of media that will not, and the safe handling of equipment that is recycled, returned to a lessor, or sold. Disposal is the goal. The methods are how you get there. What Is Secure Data Destruction? Secure data destruction is the subset of disposal that renders media permanently unusable or its contents mathematically irretrievable. Shredding a drive, pulverising it, incinerating it, or destroying the encryption keys that make an encrypted disk readable are all forms of destruction. Destruction is one route to disposal, and it is the right route when the data is highly sensitive, or the media will never be reused. Secure Data Disposal vs. Secure Data Destruction: What Is the Difference? The distinction matters more than it looks. Disposal is the outcome you owe to every framework: data gone, unrecoverable, equipment handled appropriately. Destruction is just one of the methods. You can dispose of data without destroying the hardware by sanitising a drive thoroughly enough to reuse it. Confusing the two leads to two classic mistakes: destroying assets that could have been securely wiped and reused, and assuming a quick deletion counts as disposal when it does not. Important: Emptying the recycle bin, formatting a drive, or hitting delete does not dispose of data under any of these frameworks. Standard deletion only removes the pointer to the data; the bits remain until they are overwritten. Every framework discussed here expects the data to be unrecoverable, which is a far higher bar than not visible. What ISO 27001 Requires for Secure Data Disposal ISO/IEC 27001 handles disposal through a small cluster of Annex A controls that auditors read as a single process rather than in isolation. The two controls that do most of the work are 7.14 and 8.10. For a deeper look at how these controls fit into a broader compliance program, see our ISO 27001 implementation guide. ISO 27001 Annex A 7.14: Secure Disposal or Re-Use of Equipment Annex A 7.14 is a physical control. Before any equipment is disposed of or reused, the organisation must check whether it holds information assets or licensed software and ensure those are permanently erased or the media physically destroyed. It applies to servers, laptops, desktops, mobile devices, printers, network gear, and any storage media: if it ever processed information, it is in scope. The control replaces the older 2013 clause 11.2.7 and adds explicit expectations around removing identifying markings and handling end-of-occupancy scenarios. ISO 27001 Control 8.10: Information Deletion Annex A 8.10 is a technological control, and it focuses on the data rather than the box. It requires information stored in systems, devices, or media to be deleted when it is no longer required, and rendered unrecoverable. The cleanest way to keep these straight: 8.10 governs the data while it is in use or reaches its retention limit; 7.14 governs the hardware at end of life. Most retention-driven deletion sits under 8.10; most decommissioning sits under 7.14. ISO 27001 Control 8.12: Data Leakage Prevention and Its Role in Disposal Control 8.12 is rarely filed under disposal, but improperly discarded media is one of the oldest data leakage channels there is. A drive that leaves your control with recoverable data on it is a leak, regardless of how it left. Treating disposal as part of your leakage prevention posture forces the right question at the right time: what could walk out the door on this device, and has it actually been removed? Physical Destruction and Irretrievable Erasure Under ISO 27001 ISO 27001 offers two broad routes: physically destroy media that holds information, or erase and overwrite it so retrieval by a malicious party is precluded. The standard cross-references ISO/IEC 27040 for detailed sanitisation methods. The unifying requirement is that recovery should be impractical, not merely inconvenient. Deletion alone never satisfies this. Overwriting, Full-Disk Encryption, and Other Approved Methods Overwriting user-accessible storage with multiple passes is acceptable for many sensitivity levels. Full-disk encryption changes the economics of disposal entirely: if a device is encrypted from day one and the keys are properly managed, secure disposal can be as simple as destroying the keys, a technique known as
A business continuity plan that has never been tested is, to a SOC 2 auditor, a document and nothing more. The Availability criteria do not award credit for a polished plan sitting in a shared drive. They ask for evidence that you ran the plan, watched it work or fail, recorded what happened, and fixed what broke. That gap — between having a plan and proving it works — is where most availability findings originate. Business continuity plan testing for SOC 2 is the exercise that turns your plan into auditable evidence. It maps directly to Availability criterion A1.3, one of the few SOC 2 controls that explicitly requires you to test something rather than merely document it. This guide covers what counts as a valid test, the test types auditors accept, a step-by-step process, the exact evidence you need, and the mistakes that turn a routine review into a finding. What Is Business Continuity Plan Testing in the Context of SOC 2? Business continuity plan (BCP) testing is the structured validation of whether your organization can keep critical operations running — and restore them within defined targets — during a disruption. In a SOC 2 context, the testing is not freeform. It must produce dated, traceable evidence that the recovery procedures in your plan actually work, that the people involved know their roles, and that systems and data come back within your stated recovery objectives. Why SOC 2 Requires Business Continuity Plan Testing SOC 2 is an attestation against the AICPA’s Trust Services Criteria, and the Availability category exists specifically for organizations that make uptime or resilience commitments to customers. A plan you never exercise cannot demonstrate operating effectiveness over the audit period — which is the entire point of a Type 2 examination. Testing is the control that converts a static plan into a recurring, observable activity an auditor can sample. SOC 2 Trust Services Criteria and BCP Testing Requirements Availability is one of the five Trust Services Criteria, and it is optional, included only when your service commitments warrant it. When in scope, it is built around three sub-criteria: A1.1 addresses capacity management. A1.2 addresses recovery infrastructure and backup processes. A1.3 addresses the testing of recovery procedures. BCP testing lives squarely in A1.3, with A1.2 supplying the backups and infrastructure that the test validates. Availability Criteria A1.2 and A1.3 Explained Per the AICPA’s Trust Services Criteria, A1.2 requires the entity to design, implement, operate, and monitor environmental protections, recovery infrastructure, and data backup processes that meet its availability objectives. In plain terms: you need real backups, stored away from production, with recovery infrastructure ready to use. A1.3 then requires the entity to test recovery plan procedures supporting system recovery to meet its objectives. The two work as a pair: A1.2 builds the capability, A1.3 proves it functions. Important: The most common A1.3 gap is not a missing test. It is a test that never validated the recovery objectives. Teams run a tabletop, write “no issues found,” and move on — but the plan claims a 4-hour RTO that no one ever measured against an actual restore. If your plan states recovery targets, your test evidence must show whether you met them. A test that does not measure against your RTO and RPO leaves the most important question unanswered. What Auditors Look for During a BCP Test Review Auditors want proof that the test happened, proof that it was meaningful, and proof that it led somewhere. Concretely, that means a test plan with a defined scenario, a dated record of execution with participants, results measured against your recovery objectives, a list of gaps or issues found, and evidence that those issues were remediated. A test that finds nothing and changes nothing is treated with suspicion — because real tests almost always surface something. Types of Business Continuity Plan Tests Accepted for SOC 2 SOC 2 does not mandate a specific test type. It expects the rigor of the test to match the criticality of what you are protecting. The four common approaches sit on a spectrum from low-effort, low-disruption to high-effort, high-assurance. Tabletop Exercises A tabletop exercise is a facilitated discussion where key personnel talk through a disruption scenario and their responses. It is cheap, fast, and excellent for confirming that people understand their roles and that the plan reads coherently. Its limit is obvious: nobody actually recovers anything. For many organizations a tabletop is a legitimate annual test, especially in the first audit cycle, but auditors expect more rigor as a program matures. Walkthrough and Simulation Tests A simulation applies a specific scenario and asks the team to perform recovery actions, not just describe them. It is more involved than a tabletop and far better at exposing the gaps that only appear when people touch the tools. Simulations are where teams discover that a runbook references a system that was decommissioned, or that the on-call engineer lacks the access the plan assumes. Full Interruption Tests A full interruption test shuts down primary systems and shifts operations entirely to the recovery environment. It is the most comprehensive validation available and the only one that proves your failover genuinely works end to end. It also carries real operational risk, so it demands thorough planning and is usually reserved for mature programs and the most critical systems. Parallel Testing Parallel testing activates recovery systems alongside production without taking the primary offline, then compares the two to confirm the recovery environment performs as expected. It delivers much of the assurance of a full interruption test while sparing the business the disruption. For most SaaS and cloud-hosted services, parallel testing of failover and restore is the sweet spot between confidence and risk. How to Test Your Business Continuity Plan for SOC 2 Compliance The sequence below aligns with the contingency planning process in NIST’s Contingency Planning Guide, SP 800-34, which auditors widely treat as authoritative for resilience practices. Each step produces an artifact, and the artifacts together form

31% of organizations have caught former employees accessing SaaS applications after their departure (source). Seventy percent of intellectual property theft happens in the ninety days surrounding a resignation announcement. The pattern is so consistent that auditors now treat termination day as one of the highest-risk windows on the security calendar. This article is a working employee offboarding checklist for IT, security, and HR teams who want to close that window cleanly. It walks through ten steps that revoke access without leaving gaps, then covers edge cases (remote workers, hostile exits, lost devices), the manual-versus-automation tradeoff, and post-offboarding monitoring. Use it as a baseline and adapt it to your environment. What Is Employee Offboarding and Why Does Access Revocation Matter? Employee offboarding is the structured process of separating a person from an organization: removing their access, recovering company property, documenting their exit, and updating records. The access revocation piece is the part where most programs fail quietly. Accounts get disabled in the identity provider but stay active in a dozen SaaS tools. Badges get collected but VPN tokens stay valid. The person is gone; the keys to the building are not. Why Employee Offboarding Is a Critical Security Risk Offboarding fails because access has multiplied faster than the processes designed to manage it. The average enterprise now operates somewhere between 275 and 660 SaaS applications depending on size, with employees touching dozens of them each week. Each application is a separate place that needs to be cleaned up, and each one creates an independent point of failure. The departing employee is a particularly acute version of this risk because the motivation to walk away with something often peaks during the same window that access is supposed to be revoked. The Cost of Leaving Access Open After Departure The financial picture is well documented. The 2025 Ponemon Cost of Insider Risks report puts the average annual cost of insider-related incidents at $17.4 million per organization, with containment taking an average of 81 days. Even when a departed employee never actively misuses their access, the existence of a forgotten account is enough to compromise a SOC 2 audit, trigger a breach notification, or create the credentialed beachhead that an outside attacker eventually exploits. The cases keep appearing. Cash App was breached in 2022 when a former employee accessed the records of 8 million customers after leaving. In May 2024, FinWise Bank disclosed that a former employee accessed internal systems after departure because access had never been fully revoked. Intel sued a former engineer in 2024 for downloading roughly 18,000 sensitive files in the days before he left. Ponemon’s 2025 report found that containment costs scale steeply with time. Incidents resolved in under 30 days averaged about $11 million, while those over 90 days averaged $17 million. The biggest variable is not detection capability. It is how fast access actually came down on day one. Compliance and Legal Implications of Incomplete Offboarding Access revocation is not a “best practice.” It is an explicit control requirement in nearly every framework against which an organization is likely to be audited. NIST SP 800-53 control PS-4 requires that on termination, organizations disable system access within an organization-defined time period, terminate or revoke any authenticators, and retrieve organizational property. ISO/IEC 27001 includes equivalent expectations under its Annex A controls for termination of employment. The AICPA Trust Services Criteria for SOC 2 cover this under Common Criteria CC6.2 and CC6.3, and auditors routinely pull a sample of terminated employees and verify timestamps in the identity provider against the HR system. GDPR adds a separate dimension. If a former employee still has access to the personal data of EU residents, that constitutes unauthorised processing under Article 32, and it is the controller’s responsibility, regardless of intent. HIPAA does the same for protected health information. Whatever the framework, the question an auditor or regulator will ask is the same: how quickly was access revoked, and can you prove it? Who Is Responsible for Employee Offboarding? Offboarding fails most often because no one owns the whole process. Four groups need to be in the loop, and each one has a distinct job. HR and People Operations HR is the source of truth for the termination event. Their job is to capture notice of departure, set the official last day, communicate timing to the rest of the business, and serve as the trigger that starts every downstream task. If HR does not record the termination in the HRIS, nothing automated will fire. IT and Security Teams IT executes the access teardown. They disable accounts in the identity provider, revoke SSO and OAuth tokens, remove SaaS application access, suspend email, and recover devices. Security teams typically run the audit trail and post-offboarding monitoring, and they are the ones answering when an account flagged six months later turns out to belong to a person who left in March. Legal and Compliance Legal handles NDA reminders, IP assignment confirmations, non-disclosure obligations, and any contractual surprises. Compliance owns the documentation: the evidence trail that proves the offboarding actually happened and met the relevant control requirements. For regulated industries this becomes audit evidence; for everyone else it becomes legal cover. Direct Managers Managers know things HR does not. They know which shared drives the person owned, which third-party vendors they had standing access to, which client passwords they may have rotated themselves, and which projects need a transition plan. A solid offboarding process forces the manager into the workflow with a checklist of role-specific items, because no central team can guess them. Employee Offboarding Checklist: 10 Steps to Revoke Access Without Leaving Gaps This is the core sequence. The order matters: starting with notification and inventory before disabling accounts means you do not lock the person out of a system you still need them to hand off. Step 1: Initiate Offboarding Immediately Upon Notice of Departure The moment notice is given — resignation, termination decision, or end of contract — the offboarding workflow should start. This means

Plenty of companies treat an ISO 27001 certificate as proof of GDPR compliance. It is not. The two frameworks overlap heavily, but they answer different questions, and the gap between them is exactly where regulators tend to look. ISO 27001 tells you how to build a defensible security program. GDPR tells you what the law expects when that program touches personal data. Run one without understanding the other, and you will either over-engineer security you do not strictly need, or miss privacy obligations that carry real financial exposure. This article maps where ISO 27001 and GDPR meet, where they part ways, and how to run them as a single coordinated effort rather than two competing projects. What Is ISO 27001? ISO/IEC 27001 is the international standard for an Information Security Management System, or ISMS. The current edition is ISO 27001:2022. It is not a checklist of technical fixes. It is a management framework: a structured, repeatable way to identify information security risks, decide how to treat them, document those decisions, and improve over time. Clauses 4 to 10 of the standard define the mandatory ISMS requirements, covering leadership, risk assessment, internal audit, and management review. Annex A then lists 93 controls grouped into four themes: organisational, people, physical, and technological. You do not implement all 93 by default. You select the controls that address your assessed risks and justify your choices in a document called the Statement of Applicability. Certification against ISO 27001 is voluntary and is granted by an accredited third-party body after an audit. What Is GDPR? The General Data Protection Regulation is European Union law. It has been applied since 25 May 2018, and it applies to any organisation that processes the personal data of people in the EU, wherever that organisation is based. GDPR is fundamentally about the rights of individuals, not just the security of data. It grants people rights over their personal data, including access, correction, erasure and portability. It places obligations on the organisations that decide how data is used (controllers) and those that process it on their behalf (processors). It requires a lawful basis for every processing activity, mandates breach notification, and demands transparency about what happens to people’s information. You do not implement GDPR and receive a certificate. You obey it, and a regulator decides whether you have. Key Differences Between ISO 27001 and GDPR Scope and Purpose ISO 27001 protects all information assets an organisation holds: intellectual property, financial records, operational data, source code and, yes, personal data. Its purpose is the confidentiality, integrity and availability of information in general. GDPR is narrower in one sense and broader in another. It covers only personal data of individuals in the EU, but it protects the person behind the data, not merely the data itself. A system can be flawlessly secure and still violate GDPR. Legal Obligation vs. Voluntary Certification This is the difference that catches people out. GDPR is binding law. If you process EU personal data, compliance is not optional, and there is no opting out. ISO 27001 is a voluntary standard. Organisations pursue it for assurance, for competitive advantage, and because customers increasingly demand it. Crucially, there is no such thing as a GDPR certificate. Regulators assess compliance through investigation and enforcement, not through a badge you can display. Penalties for Non-Compliance GDPR fines run on two tiers under Article 83. Less severe infringements — such as failures around records of processing or breach notification — can reach €10 million or 2% of global annual turnover, whichever is higher. The more serious tier, covering breaches of the core processing principles and data subject rights, can reach €20 million or 4% of global annual turnover. Failing an ISO 27001 audit carries no legal fine at all. The consequence is commercial: you do not get the certificate, or you lose it, and that can cost you contracts. How ISO 27001 and GDPR Align Despite their different purposes, the two frameworks were built on compatible logic, which is why running them together works. Both treat information security as central. GDPR Article 32 requires “appropriate technical and organisational measures” to secure personal data. That phrasing is almost a direct description of what an ISO 27001 ISMS produces. The controls an organisation selects for confidentiality and access already serve the regulation’s security expectations. Both are risk-based. ISO 27001 starts every control decision from a risk assessment. GDPR expects the same proportionality: the measures you apply should match the sensitivity of the data and the likelihood and severity of harm. One risk methodology can serve both, provided you assess personal data processing risks alongside broader security risks. Both demand incident response. ISO 27001’s incident management controls require organisations to detect, assess and respond to security events. GDPR Article 33 requires notifying the supervisory authority of a personal data breach within 72 hours of becoming aware of it. The ISO process is the engine that makes the GDPR deadline achievable. How ISO 27001 Can Help You Comply With GDPR Four areas of an ISMS do direct, practical work toward GDPR compliance. Asset management. ISO 27001 requires an inventory of information and associated assets, with owners assigned. You cannot protect personal data, respond to access requests, or maintain records of processing if you do not know where that data lives. The asset inventory is the foundation for both frameworks. Access control. Identity management, privileged access controls and the principle of least privilege limit who can see personal data. That directly supports the GDPR requirement to ensure confidentiality and to prevent unauthorised access. Operational security. Logging, malware protection, backup and secure configuration keep personal data accurate, available and resistant to compromise. These map cleanly onto the integrity and availability expectations in Article 32. Techniques such as data masking for GDPR and ISO 27001 also sit within this space, reducing exposure without sacrificing operational utility. Incident management. A defined process for detecting and handling security events gives you the evidence trail and the response capability you need to

A company that already holds a SOC 2 report has, by most industry estimates, already built somewhere between 60 and 80 percent of what ISO 27001 certification requires. Yet only a small fraction of organizations actually capture that overlap. Teams run the second framework as a fresh project, rewrite policies that already exist, and re-collect evidence they already have on file. The result is paying twice for the same security program. SOC 2 to ISO 27001 mapping is the discipline that stops this. It is a control crosswalk: a structured comparison that shows which SOC 2 controls already satisfy which ISO 27001 requirements, where the genuine gaps sit, and what new work the second framework actually demands. Done well, it turns the second audit from a rebuild into a mapping exercise. What Is SOC 2 to ISO 27001 Mapping? SOC 2 to ISO 27001 mapping links each SOC 2 Trust Services Criterion to its corresponding ISO 27001 clause or Annex A control. The output is a single control library: each control is defined once, tagged to both frameworks, and backed by evidence that both auditors will accept. Worth being clear about upfront: a crosswalk does not make you compliant with anything. It shows where coverage already exists and where it does not. The real work still sits in control design, evidence discipline, and keeping the mapping current as systems and vendors change. A spreadsheet built once and never touched again becomes an audit liability, not an asset. For a structured starting point, a thorough SOC 2 to ISO 27001 gap analysis will surface those liabilities before an auditor does. SOC 2 Trust Services Criteria: An Overview SOC 2 is an attestation framework from the American Institute of Certified Public Accountants (AICPA). It is built on five Trust Services Categories: Security, Availability, Processing Integrity, Confidentiality, and Privacy. Security is the only mandatory category, and every SOC 2 report includes it. The Security category is evaluated through the Common Criteria, written as CC1 through CC9, containing 32 individual criteria in total. CC1 through CC5 cover the control environment, communication, risk assessment, monitoring, and control activities, and they align directly with the COSO internal control framework. CC6 through CC9 are more technology-specific, covering logical and physical access, system operations, change management, and risk mitigation. A SOC 2 audit produces one of two report types. A Type 1 report assesses control design at a single point in time. A Type 2 report assesses both design and operating effectiveness across an observation window, usually 3 to 12 months. A licensed CPA firm issues the report. SOC 2 is an attestation, not a certification, and there is no such thing as a SOC 2 certificate. ISO 27001 Annex A Controls: An Overview ISO/IEC 27001 is the international standard for an information security management system, or ISMS. The current version, ISO 27001:2022, has two distinct layers, and the distinction matters for any mapping effort. Clauses 4 through 10 define the management system itself: organizational context, leadership, planning, risk treatment, support, operations, performance evaluation, and improvement. These clauses are mandatory. Annex A is the second layer, a reference catalogue of 93 controls grouped into four themes: Organizational (37 controls), People (8), Physical (14), and Technological (34). The 2022 revision consolidated the previous 114 controls and 14 domains and added 11 new controls covering areas such as threat intelligence and cloud security. Annex A controls are not all mandatory. Organizations select controls based on a risk assessment and record their choices, including any exclusions and the reasoning behind them, in a Statement of Applicability. Certification is granted by an accredited body, lasts three years, and requires annual surveillance audits. Learn more about what the full certification process involves. Key Structural Differences That Affect Mapping The two frameworks share a large security foundation, but they are built differently, and a mapping that ignores the structural gaps will fail. Understanding ISO 27001 vs SOC 2 at a structural level is the prerequisite for any mapping work worth doing. Four differences matter most. ISO 27001 certifies a management system, while SOC 2 attests to a set of controls. ISO Clauses 4 through 10 have no direct SOC 2 equivalent, because SOC 2 never asks you to prove you run a continuous, governed program; it asks only whether specific controls met specific criteria during the review period. Scope differs too. An ISO 27001 ISMS is expected to cover the organization broadly, while SOC 2 scope is set at the level of a system or service. The outputs differ as well: ISO produces a pass or fail certificate, whereas a SOC 2 report can carry noted exceptions or a qualified opinion and still be a valid, useful report. And because SOC 2 Type 2 tests evidence across a defined window, a control that worked only on audit day will not pass. The most common mapping mistake is treating ISO 27001 as SOC 2 plus a few extra controls. It is not. The Annex A controls map cleanly, but the ISMS management clauses, including internal audit, management review, and continual improvement, are a separate body of work with no SOC 2 starting point. Budget for them as net-new. SOC 2 Common Criteria to ISO 27001 Control Mapping The Common Criteria map to ISO 27001 with a high degree of overlap. The table below is a practical starting crosswalk for the CC series. It lists the primary ISO 27001 references rather than every possible match, and your auditor’s judgment will shape the final mapping. SOC 2 Common Criteria Topic Primary ISO 27001:2022 References CC1 Control Environment Clauses 5 (Leadership), 6 (Planning), A.5.1, A.5.2, A.6.1–A.6.4 CC2 Communication and Information Clause 7.4 (Communication), A.5.1, A.6.3, A.8.2 CC3 Risk Assessment Clause 6.1 (Risk Assessment), A.5.7, A.8.8 CC4 Monitoring Activities Clause 9 (Performance Evaluation), A.5.35, A.5.36, A.8.16 CC5 Control Activities Clause 6.1.3 (Risk Treatment), A.5.37, A.8.9 CC6 Logical and Physical Access A.5.15–A.5.18, A.5.31, A.7.1–A.7.4, A.8.2–A.8.5, A.8.18 CC7 System Operations and Incident Response A.5.24–A.5.28, A.8.15, A.8.16 CC8
AI Hub
The latest insights into AI implementation and compliance
Most organizations think their AI governance is further along than it is. McKinsey’s 2026 AI Trust Maturity Survey of roughly 500 organizations found an average maturity score of 2.3 out of 4, and only about a third reported level three or higher in strategy, governance, and agentic AI oversight. Adoption is outpacing control, and regulators have noticed. An AI governance maturity model gives you a way to measure that gap honestly. This guide covers what a maturity model is, the six dimensions it should measure, the five levels most models use, and how to assess your own organization and build a roadmap to the next level. What Is an AI Governance Maturity Model? An AI governance maturity model is a structured framework that describes how capable an organization is at governing its AI systems, usually across five progressive levels. The concept borrows directly from the Capability Maturity Model (CMM) that software engineering has used since the early 1990s: define the capability, describe what it looks like at each stage of development, and score yourself against it. The purpose is diagnosis. A maturity model tells you where governance is strong, where it’s theater, and where it doesn’t exist at all. How It Differs from General AI Governance Frameworks Frameworks like the NIST AI Risk Management Framework or ISO/IEC 42001 tell you what good governance contains: policies, risk assessments, accountability structures, monitoring. A maturity model tells you how well you’re doing those things today. The framework is the destination. The maturity model is the odometer. That distinction matters in practice. Plenty of companies can point to an AI policy document. Far fewer can show that the policy changes what teams actually ship. Why Enterprises Need a Maturity Model Three reasons. First, budget: you can’t prioritize governance investment without knowing which dimension lags. Second, accountability: a maturity score gives boards something concrete to track quarter over quarter. Third, regulation: the EU AI Act and frameworks like ISO 42001 assume a functioning management system, and a maturity assessment is the fastest way to find out whether yours would survive scrutiny. Core Dimensions of an AI Governance Maturity Model A useful model measures more than policy coverage. Six dimensions show up consistently across the credible models, including the IEEE-USA flexible maturity model built on the NIST AI RMF. Strategy and leadership. Does the organization have a stated position on AI risk, an executive owner (increasingly a Chief AI Officer), and board visibility? Gartner’s 2025 polling found 55% of organizations now have an AI board or dedicated oversight committee, which means nearly half still govern by improvisation. Policies, standards, and accountability. Written policies mapped to regulations, a RACI matrix for AI decisions, and clear escalation paths. Many organizations adapt the three lines of defense model from financial risk: the teams building AI, the risk function overseeing them, and internal audit checking both. Data governance and model lifecycle. Training data lineage, quality controls, and lifecycle management from development through deployment, monitoring, and retirement. This is where AI governance meets MLOps, and where mature organizations maintain an AI register, a live inventory of every model and system in production. Risk, compliance, and ethics. Risk classification of AI systems, impact assessments, bias and fairness testing, and explainability requirements. Banks will recognize the DNA of model risk management under SR 11-7 here. People, skills, and culture. Training, role clarity, and whether people outside the governance team actually understand their obligations. Tools, automation, and monitoring. Drift detection, automated policy checks, audit logging, and dashboards. Governance that lives in spreadsheets caps out around level three. The 5 Levels of AI Governance Maturity Level 1: Ad Hoc / Initial AI use happens without oversight. There’s no inventory, no policy, or a policy nobody follows. Shadow AI is common, and risk surfaces only when something breaks publicly. Level 2: Developing / Repeatable Someone has been assigned responsibility. A draft policy exists, a partial inventory exists, and reviews happen for high-profile projects. The practices are repeatable but depend on specific people rather than defined processes. Level 3: Defined / Structured Governance is documented, standardized, and applied across the organization. There’s a governance committee, a risk classification scheme, defined lifecycle gates, and mandatory training. Most organizations pursuing ISO 42001 certification are working to reach and formalize this level. Level 4: Managed / Metrics-Driven Governance produces numbers. Coverage rates, review cycle times, incident counts, and risk reduction are measured and reported to leadership. Controls are enforced by tooling rather than goodwill, and audits confirm the system works as described. Level 5: Optimized / Adaptive Governance improves itself. Monitoring feeds back into policy, controls adapt to new model types (agentic systems being the current test), and the organization anticipates regulatory change rather than reacting to it. Almost nobody is here yet, and that’s fine. Level 5 is a direction, not a deadline. Insider Note: In assessments, the most common self-scoring error is claiming level 3 on the strength of documents alone. If your policy says every model gets a pre-deployment review and your inventory shows 40 models but your review log shows 6, you’re at level 2. Evidence beats paperwork every time, and auditors check the logs first. AI Governance Maturity Matrix The matrix crosses dimensions with levels so you can score each one independently. Organizations are rarely uniform: it’s normal to sit at level 3 on policy and level 1 on monitoring. For scoring, keep the rubric simple: 1 to 5 per dimension, scored on evidence you could show an auditor, not on intentions. Board-level indicators (does the board see AI risk reporting?) and operational indicators (does every production model have a completed impact assessment?) should be scored separately, because they fail independently. How to Assess Your Current AI Governance Maturity Start with a baseline self-assessment. Pull together a cross-functional group covering engineering, legal, risk, security, and the business owners of major AI use cases, and score each dimension against the matrix. Half a day is usually enough for a first pass. For each dimension, the
An AI agent that can read your inbox, query your CRM, and dig through internal documents has more standing access than most of your employees. It handles sensitive data, acts on its own, and often passes that data through sub-processors you’ll never see. Certifications are the quickest way to tell which vendors have let an outsider check their work, and which ones just put the word “secure” on a landing page. No single certificate proves an AI agent is safe. But the right mix of security attestations, privacy certifications, and AI governance standards tells you the vendor has real controls, that an independent auditor has tested them, and that someone is on the hook when the agent misbehaves. This guide covers which certifications to ask for, how to verify them, and which claims should make you walk away. The Core Certifications Every Secure AI Agent Vendor Should Hold SOC 2 Type II SOC 2 Type II is the baseline for any SaaS or AI vendor that handles customer data. A licensed CPA firm audits the vendor against the AICPA’s Trust Services Criteria (Security, Availability, Processing Integrity, Confidentiality, and Privacy) and reports on whether its controls actually worked over a review period, usually 3 to 12 months. A Type I report only confirms the controls existed on one particular day. For an AI agent vendor, insist on Type II. Anything less tells you nothing about how the company runs day-to-day. ISO/IEC 27001 ISO/IEC 27001 certifies that the vendor runs a formal information security management system (ISMS): documented risk assessments, defined controls, internal audits, and management review, all verified by an accredited certification body. It’s the most widely recognized security certification outside the US and often a hard procurement requirement in Europe, the UK, and the Gulf. A vendor with international customers should hold it alongside SOC 2, not instead of it. ISO/IEC 27701 (Privacy Information Management) ISO/IEC 27701 extends ISO 27001 with a privacy information management system (PIMS). It maps closely to GDPR concepts like controller and processor obligations, consent, and data subject rights. Almost every AI agent processes personal data at scale, and ISO 27701 is a decent signal that the vendor has built privacy into how it operates instead of delegating it to a policy PDF. ISO/IEC 42001 (AI Management Systems) ISO/IEC 42001 is the first certifiable international standard for AI governance. According to the International Organization for Standardization, it sets out requirements for building and maintaining an AI management system (AIMS): AI risk management, AI system impact assessments, lifecycle management, and oversight of third-party suppliers. For an AI agent vendor, this is the one that covers what SOC 2 and ISO 27001 don’t: how the vendor governs model behavior, training data, and the wider impact of autonomous systems. Worth Knowing: ISO 42001 certificates only started appearing in volume in 2024, and the accreditation ecosystem is still catching up. Check that the certificate came from a certification body accredited for ISO 42001 specifically (under ANAB or UKAS, for example), not just one accredited for ISO 27001. HIPAA (for Healthcare AI Agents) If the agent touches protected health information (PHI), the vendor has to comply with the HIPAA Privacy and Security Rules and sign a Business Associate Agreement (BAA). There’s no official HIPAA certification, so vendors prove compliance through third-party assessments, a SOC 2 with HIPAA mapping, or HITRUST CSF certification. A vendor that won’t sign a BAA has disqualified itself for healthcare work. PCI DSS (for Payment-Handling AI Agents) AI agents that process, store, or transmit cardholder data (think agents automating billing, refunds, or checkout) fall under PCI DSS. Ask for the vendor’s Attestation of Compliance (AOC) and check whether a Qualified Security Assessor validated it or the vendor assessed itself. The current version is PCI DSS 4.x, so an AOC that still references 3.2.1 is out of date. FedRAMP (for Government-Facing AI Agents) FedRAMP authorization is mandatory for cloud services sold to US federal agencies. Authorizations come at Low, Moderate, and High impact levels, and every authorized service appears on the public FedRAMP Marketplace. If a vendor claims FedRAMP status and isn’t in the Marketplace, either the claim is false or the service is still “in process,” and those are very different things. State and local buyers should look for StateRAMP instead. Worth Knowing: ISO 42001 Certificates ISO 42001 certificates only started appearing in volume in 2024, and the accreditation ecosystem is still catching up. Check that the certificate came from a certification body accredited for ISO 42001 specifically (under ANAB or UKAS, for example), not just one accredited for ISO 27001. HIPAA (for Healthcare AI Agents) If the agent touches protected health information (PHI), the vendor has to comply with the HIPAA Privacy and Security Rules and sign a Business Associate Agreement (BAA). There’s no official HIPAA certification, so vendors prove compliance through third-party assessments, a SOC 2 with HIPAA mapping, or HITRUST CSF certification. A vendor that won’t sign a BAA has disqualified itself for healthcare work. PCI DSS (for Payment-Handling AI Agents) AI agents that process, store, or transmit cardholder data (think agents automating billing, refunds, or checkout) fall under PCI DSS. Ask for the vendor’s Attestation of Compliance (AOC) and check whether a Qualified Security Assessor validated it or the vendor assessed itself. The current version is PCI DSS 4.x, so an AOC that still references 3.2.1 is out of date. FedRAMP (for Government-Facing AI Agents) FedRAMP authorization is mandatory for cloud services sold to US federal agencies. Authorizations come at Low, Moderate, and High impact levels, and every authorized service appears on the public FedRAMP Marketplace. If a vendor claims FedRAMP status and isn’t in the Marketplace, either the claim is false or the service is still “in process,” and those are very different things. State and local buyers should look for StateRAMP instead. Regulatory Frameworks AI Agent Vendors Must Comply With Certifications are voluntary. Regulations aren’t. A credible AI agent vendor should be able to explain, in writing, how it meets
One in five organizations has already suffered a breach traced back to shadow AI. Meanwhile, 63% of breached organizations either have no AI governance policy at all or are still drafting one. Below is a complete, copy-ready shadow AI policy template with twelve sections, plus guidance on adapting it for your company size, your industry, and the regulatory frameworks you answer to. The template assumes one hard truth up front: your employees are already using unapproved AI tools. A policy that pretends adoption hasn’t started yet fails on day one, so this one starts from the assumption that it has. What Is a Shadow AI Policy? A shadow AI policy is a formal document that defines how your organization discovers, evaluates, approves, and governs AI tools that employees adopt outside official IT channels. The term borrows from shadow IT, the older problem of unsanctioned software and hardware, but the AI version carries sharper risks: data pasted into a public model may be retained, used for training, or exposed in ways the organization can’t reverse. The policy does three jobs: it separates approved use from unapproved use, gives employees a fast and visible way to request new tools so the sanctioned route beats the workaround, and spells out what happens when someone crosses the line, including how the organization detects it and responds. Shadow AI Policy vs. General AI Acceptable Use Policy Many organizations already have an AI acceptable use policy (AUP) and assume it covers shadow AI. It usually doesn’t. An AUP tells employees how to behave inside approved tools. A shadow AI policy governs the tools themselves: which ones exist in your environment, which ones are allowed, and what happens with the rest. You need both. The AUP handles conduct; the shadow AI policy handles inventory and control. If you only have room for one document, fold the AUP’s data-handling rules into Section 6 of the template below. The Shadow AI Policy Template (Download Link and Copy-Ready Sections) We’ve created a compliance safe template for Shadow AI Policy, use the link below to create a copy and customize for your company: Download The Shadow AI Policy Template → Copy the sections below into your policy management system and replace the bracketed placeholders. The language is plain on purpose. Legalese gets skimmed. Section 1: Purpose and Scope This policy governs the acquisition, approval, and use of artificial intelligence tools, features, and services at [Company]. It applies to all employees, contractors, interns, and third parties with access to [Company] systems or data. It covers standalone AI applications, AI features embedded in existing software, browser extensions, AI agents, APIs, and personal AI accounts used for work purposes, on both corporate and personal devices. The purpose of this policy is to enable productive AI use while protecting [Company] data, customers, and legal obligations. This policy does not prohibit AI. It prohibits ungoverned AI. That last sentence matters. Employees read the purpose statement first, and it decides whether they see the policy as an enabler or a blocker. Section 2: Definitions and Terminology Shadow AI: any AI tool, feature, agent, or service used for work purposes without formal approval under this policy. Approved AI Tool: an AI tool listed in the Approved AI Tools Registry (Section 4) and used under a [Company]-managed account. Personal AI Account: an account on any AI service registered to a personal email address or paid for personally. AI Feature: AI functionality embedded within otherwise approved software (e.g., an AI assistant added to a project management tool), which requires separate evaluation. Sensitive Data: data classified as [Confidential] or [Restricted] under [Company]‘s data classification policy, including the prohibited data classes in Section 6. Define “AI feature” explicitly. Vendors now ship AI additions into already-approved SaaS products every month, and without this definition, those features inherit approval they never earned. Section 3: Roles and Responsibilities The CISO (or designated security lead) owns this policy, maintains the Approved AI Tools Registry, and runs the approval workflow. Department heads ensure their teams know the policy and surface tool requests rather than suppressing them. Legal and Compliance review tools that touch regulated data or fall under the EU AI Act, GDPR, HIPAA, or client contractual restrictions. IT operates detection and monitoring controls (Section 9). Every employee is responsible for using only approved tools for work, reporting unapproved AI use they discover, and requesting new tools through the workflow in Section 7 rather than adopting them directly. Insider Note: In organizations under roughly 200 people, the “CISO” in this section is often the same overworked IT lead who manages laptops. Name a real person, not a title that doesn’t exist yet. A policy that assigns duties to a phantom role is unenforceable, and auditors notice. Section 4: Approved AI Tools Registry [Company] maintains a registry of approved AI tools at [location/URL]. For each tool, the registry records: tool name and vendor, approved use cases, prohibited use cases, permitted data classes, account type (enterprise/team/individual), data retention and training settings, risk tier (Section 5), approval date, and next review date. Only tools listed in the registry may be used for work. Tools not listed are unapproved by default. The registry is reviewed [quarterly]. Keep the registry somewhere employees actually look, such as your intranet homepage or IT help center, not buried in a GRC platform they can’t access. An invisible registry recreates the problem the policy exists to fix. Section 5: Risk Tier Classification (Low, Medium, High) Each tool in the registry is assigned a risk tier. Low: the tool processes only public or internal non-sensitive data, runs under an enterprise agreement with training opt-out, and produces output that a human reviews before use. Approval by IT Security alone. Medium: the tool processes internal business data or connects to [Company] systems via API or integration. Approval by IT Security plus the data owner. High: the tool processes sensitive data, customer personal data, or regulated data; makes or influences consequential decisions (hiring, credit, medical, legal); or operates autonomously
Legacy threat modeling frameworks such as STRIDE were designed for software that behaves the same way over and over again. Agentic AI does no such thing. It can rewrite its own plan mid-task, call external tools, negotiate with other agents, and produce a different output from identical input. MAESTRO exists because none of the legacy threat modeling frameworks were built to handle that. MAESTRO stands for Multi-Agent Environment, Security, Threat, Risk, and Outcome. It is a seven-layer threat modeling framework created specifically for agentic AI systems, and it has become the closest thing the industry has to a standard method for reasoning about agent security. Understanding MAESTRO in the Context of Agentic AI What MAESTRO Stands For Each word in the acronym carries meaning. Multi-Agent Environment signals that the framework models entire ecosystems of interacting agents, not a single model behind an API. Security, Threat, Risk covers the core discipline: identifying attack surfaces, cataloging threats, and assessing likelihood and impact. Outcome is the part most frameworks skip. MAESTRO asks what an attack actually produces in the real world, because an autonomous agent with tool access turns a compromised prompt into a compromised action. The Origin of MAESTRO (Cloud Security Alliance) The Cloud Security Alliance published MAESTRO in February 2025. Its creator is Ken Huang, Co-Chair of the CSA AI Safety Working Groups and CEO of DistributedApps.ai. The CSA has since applied the framework publicly to real systems, including OpenAI’s Responses API and Google’s A2A protocol, which gives practitioners worked examples rather than just theory. The framework is openly published, and the CSA maintains an official companion tool, the MAESTRO Threat Analyzer, on GitHub. SOC 2, ISO 27001 and HIPAA done for you. Fixed fee, 100% audit pass rate. Audit-ready in 6 weeks. Not 6 months. Schedule Free Assessment Why Traditional Frameworks Fall Short for Agentic AI STRIDE, PASTA, LINDDUN, and OCTAVE all share a founding assumption: the system under analysis follows predictable logic with clearly defined boundaries. You draw the data flow diagram, mark the trust boundaries, and enumerate threats against components that behave deterministically. Agentic AI breaks every part of that assumption. Unique Security Challenges of Autonomous Agents Agents introduce three properties that legacy models cannot express. Non-determinism means the same input can produce different behavior, so you cannot enumerate execution paths in advance. Autonomy means the agent makes decisions and takes actions without a human approving each step, which collapses the usual assumption that a person sits between intent and execution. And in multi-agent systems there is often no stable trust boundary: agents delegate to other agents, consume tool outputs from external servers via protocols like the Model Context Protocol (MCP), and update their own memory and goals at runtime. The Gap Between Legacy Frameworks and Agent-Based Systems The practical consequence is coverage gaps. STRIDE has no category for goal manipulation, where an attacker gradually steers what an agent is trying to achieve. PASTA assumes attacker objectives and data flows are fixed, which fails for systems that learn and adapt during operation. LINDDUN addresses privacy but says nothing about agent collusion or memory poisoning. A threat model built purely on these frameworks will pass review and still miss the attacks that matter most in an agentic deployment. How MAESTRO Addresses Agentic-Specific Risks MAESTRO does not discard the older frameworks. It extends them with a layered reference architecture, an AI-specific threat catalog for each layer, and, critically, explicit analysis of how threats propagate between layers. That cross-layer lens is the framework’s real contribution, because most serious agentic incidents are chains: poisoned data influences a model, the model misleads an agent, and the agent takes an unauthorized action three layers away from where the attack started. The Seven Layers of the MAESTRO Framework MAESTRO decomposes any agentic system into seven layers, each with its own threat landscape. Layer 1: Foundation Models The core LLMs or other models the agents reason with. Threats here include adversarial examples, model extraction, backdoored weights, and jailbreaks that bypass safety training. If the model is a third-party API, supply chain risk lives at this layer too. Layer 2: Data Operations Everything the agent ingests, stores, and retrieves: training data, RAG pipelines, vector databases, and agent memory. Data poisoning and memory tampering are the signature threats at this layer, and they are especially dangerous because a poisoned memory persists across sessions and keeps shaping future decisions long after the initial attack. Layer 3: Agent Frameworks The orchestration software that turns a model into an agent: LangChain, CrewAI, AutoGen, custom planners, and tool-calling logic. Threats include prompt injection through tool outputs, insecure tool definitions, and manipulation of the planning loop itself. Layer 4: Deployment Infrastructure The servers, containers, and cloud services the agents run on. The CSA’s threat catalog here reads like traditional cloud security with an agentic twist: compromised container images carrying malicious agent code, Kubernetes orchestration attacks, denial of service against agent runtimes, and tampering with Infrastructure-as-Code templates that provision agent resources. Layer 5: Evaluation and Observability The systems that monitor, evaluate, and debug agent behavior. This layer is often forgotten, and attackers know it. The CSA specifically flags poisoning observability data: manipulating the telemetry fed to monitoring systems so that incidents stay hidden from security teams while malicious activity continues. Layer 6: Security and Compliance MAESTRO treats this as a vertical layer that cuts across all others: identity and access management, guardrails, policy enforcement, and compliance controls. Threats include permission escalation, guardrail bypass, and compromise of the security agents themselves in architectures where AI enforces policy on other AI. Layer 7: Agent Ecosystem The environment where agents interact with users, other agents, and marketplaces. This is where the genuinely novel threats live: agent impersonation, misleading agent capability cards, tool squatting, and collusion between agents to achieve outcomes no single agent was authorized to pursue. Insider Note: In real assessments, Layers 5 and 6 expose the maturity gap fastest. Most teams’ shipping agents can describe their model and their orchestration framework in detail, then

78% of organizations have no formal policies for creating or removing AI agent identities, according to a 2026 report from the Cloud Security Alliance and Oasis Security. The same research found that 92% are not confident that their legacy identity and access management tools can handle the risks agents introduce. Those two numbers describe the problem in full: enterprises are deploying autonomous software that reads email, queries databases, and triggers actions across production systems, and most of them cannot say who authorized it, what it can touch, or how they would prove any of that to an auditor. This is not a future problem. Agents are already operating inside regulated environments governed by the GDPR, HIPAA, SOX, and the EU AI Act. Every access decision an agent makes is a compliance event, whether or not anyone is logging it. This article covers what regulators actually expect, where traditional IAM falls short, and how to build an access framework for AI agents that survives an audit. Understanding the Compliance Landscape for AI Agents Key Regulations Impacting AI Agent Access No regulation says “AI agent” and then hands you a checklist. Instead, agents inherit obligations from every framework that governs the data and systems they touch. Under the GDPR, an agent processing personal data triggers the full set of principles in Article 5: lawfulness, purpose limitation, data minimization, and accountability. If an agent makes decisions that produce legal or similarly significant effects on individuals, Article 22 restrictions on automated decision-making apply as well. HIPAA requires covered entities to implement access controls, audit controls, and integrity protections for electronic protected health information under the Security Rule, and an agent with access to ePHI is subject to the same technical safeguards as a human workforce member. SOX demands that access to financial reporting systems be controlled, segregated, and reviewable, which becomes genuinely difficult when an autonomous agent can touch the general ledger. The EU AI Act adds an AI-specific layer, and its timeline is widely misunderstood. Following the Digital Omnibus agreement, obligations for standalone high-risk systems under Annex III were deferred to December 2, 2027. But the Article 50 transparency obligations still apply from August 2, 2026, meaning agents that interact with people in the EU must disclose their artificial nature on the original schedule. Treating the Omnibus as a blanket delay is one of the most common compliance mistakes being made right now. Important: The Digital Omnibus deferred the high-risk regime, not the whole Act. If an AI agent interacts with users in the EU, the August 2, 2026, transparency requirements were not moved, and the AI Office’s enforcement powers go live on the same date. Do not stand down 2026 workstreams based on headlines about the 2027 deferral. How AI Agents Create New Compliance Risks Agents break the assumptions most compliance programs are built on. A human user requests access, receives a role, and behaves within a predictable envelope. An agent reasons about its own goals, chains tool calls across systems, and can attempt actions its designers never anticipated. It operates at machine speed and machine volume, so a misconfigured permission produces thousands of non-compliant data touches before anyone notices. And because agents frequently run on shared service accounts or borrowed OAuth tokens, attribution collapses: the audit log says the CRM was queried, but not by whom, for what purpose, or under whose authority. The Gap Between Traditional IAM Compliance and Agentic AI Traditional IAM assumes identities are stable, access needs are predictable, and behavior maps to a job description. None of that holds for agents. A 2026 Cloud Security Alliance survey found that 68% of organizations cannot reliably distinguish AI agent activity from human activity in their logs. For a compliance function, that is disqualifying. If you cannot separate agent actions from human actions, you cannot certify access, demonstrate segregation of duties, or respond to a data subject access request with confidence. Core Compliance Requirements for AI Agent Access Auditability and Traceability of Agent Actions Every major framework converges on the same demand: show your work. For agents, a login timestamp is not enough. A defensible audit trail captures the full chain of custody for each action: which agent acted, which human or process delegated the authority, which tool or API was invoked, which data was accessed, and what the outcome was. Gartner’s 2026 Market Guide for what it calls “guardian agents” describes exactly this pattern of recording agent-to-tool-to-target chains for compliance reporting and incident response. Data Protection and Privacy Obligations Agents must operate inside the same data protection perimeter as everything else. That means Data Loss Prevention (DLP) controls apply to agent outputs, not just human uploads. It means an agent’s access to personal data needs a lawful basis, documented before deployment, not reverse-engineered after. And it means retention rules follow the data into whatever context window, vector store, or scratchpad the agent moves it into. Separation of Duties in Autonomous Systems Separation of duties exists so that no single actor can both commit and conceal an error or a fraud. A single agent granted permissions across procurement, approval, and payment reconstitutes exactly the toxic combination SOX controls were designed to prevent, except now it executes at machine speed. The control translates directly: no agent should hold permission sets that a human in the same process would be prohibited from combining, and multi-agent workflows need the same conflict analysis as human role assignments. Consent, Purpose Limitation, and Data Minimization Purpose limitation is the principle that agents most naturally violate. An agent given broad access “to be helpful” will use data collected for one purpose to accomplish another, because nothing in its architecture knows the difference. Compliance-ready agent access means scoping data access to the declared purpose of the task and enforcing that scope technically rather than hoping the system prompt holds. Insider Note: In practice, the purpose limitation failures we see are rarely dramatic. They look like a support agent enriching a ticket with data pulled from the sales

When researchers found that Microsoft 365 Copilot could be tricked into leaking corporate data from a single email, the flaw got a clean public identifier: CVE-2025-32711, severity 9.3. When a bug hunter coaxed ChatGPT into producing valid Windows product keys by framing the request as a guessing game, it got nothing. Both were prompt injections. Only one is trackable. That Vulnerability Tracking Gap in AI Security, and what it costs defenders, is the subject of this article. What Is a CVE and Why Does It Matter for Software Security? A CVE (Common Vulnerabilities and Exposures) is a unique public identifier for a specific software flaw. It gives the whole industry one name for one bug, so a researcher in Berlin and an analyst in Bahrain know they mean the same thing. The Role of MITRE’s CVE Program in Traditional Vulnerability Management The CVE program is run by the MITRE Corporation, a US nonprofit. Since 1999 it has assigned hundreds of thousands of IDs, each tied to a discrete, reproducible defect in a defined product and version. A CVE is the connective tissue of coordinated disclosure: a researcher reports the flaw, the vendor patches it, the ID is published, and defenders map it to their own assets. Without that shared label, the same bug ends up with three names and no clear owner. The National Vulnerability Database (NVD) and CVSS Scoring The National Vulnerability Database, maintained by NIST, enriches each CVE with a CVSS (Common Vulnerability Scoring System) score from 0 to 10. That lets teams triage: a 9.3 jumps the queue, a 4.0 waits. Why Prompt Injection Breaks the Traditional CVE Model The CVE model assumes a bug lives in code, sits in a version, and can be fixed. Prompt injection violates all three. Prompt Injection as a Class of Attack, Not a Discrete Bug Prompt injection smuggles instructions into the data an LLM reads, so the model follows the attacker rather than the user. OWASP ranks it as LLM01, the top entry in its 2025 Top 10 for LLM Applications. It is a property of how language models work, not one line of faulty code, so you cannot file a CVE against it. A SQL injection either works or it does not. A prompt injection might succeed nine times in ten, fail on the eleventh, then stop working after a silent model update, which makes the “reproducible” part of reporting genuinely hard. Model Versioning vs. Software Versioning Software has clean version numbers. A weight update to a hosted model can ship silently, with no version a researcher can cite. Two calls to “gpt-4o” a week apart may not behave the same way, and there is no changelog to point at. Why “Patching” an LLM Differs From Patching Code Patching code closes a specific hole. A developer rewrites the faulty line, ships the diff, and the exploit path is gone for good. That clean, binary, auditable loop is the entire premise on which the CVE system rests. “Patching” a model offers none of it. There is no single line to fix, because the behavior the attacker abused is the same behavior that makes the model useful: it reads text and follows instructions. A vendor’s only levers, retraining, hardening the system prompt, or wrapping the model in input and output guardrails, all lower the odds of a successful attack rather than removing the possibility. The fix reduces the success rate from 80 percent to 5 percent and marks it as remediated. The hole is narrower, not closed. The recent record shows how thin that margin is. EchoLeak got past Microsoft’s dedicated cross-prompt-injection classifier by hiding its exfiltration channel in reference-style Markdown that the filter did not recognize, and the AgentFlayer exploit slipped through OpenAI’s URL safety check by routing stolen data through trusted Azure Blob Storage links. Each guardrail worked against the obvious version of the attack and fell to a rephrasing. There is a tuning tax on top of that: crank the filters too tight and the model starts refusing legitimate work, so vendors settle for a balance point rather than elimination. The practical takeaway is to treat “we’ve addressed this” as risk reduction, not closure. SOC 2, ISO 27001 and HIPAA done for you. Fixed fee, 100% audit pass rate. Audit-ready in 6 weeks. Not 6 months. Schedule A Free ASSESSMENT The Current State of AI Vulnerability Tracking Several frameworks exist. None is a true registry of individual, citable prompt injection vulnerabilities. OWASP LLM Top 10 and the LLM01 Classification The OWASP GenAI Security Project’s LLM01:2025 entry is the most cited reference point. It is a category, not a catalog: it does not enumerate specific incidents with IDs. MITRE ATLAS for Adversarial AI Threats MITRE ATLAS is an ATT&CK-style knowledge base of adversarial tactics against AI systems, documenting 16 tactics and more than 80 techniques with real-world case studies as of late 2025. It maps how attacks work, but is not a per-vulnerability ledger with scores. AVID (AI Vulnerability Database) and Its Limitations AVID, run by a nonprofit, is the closest thing to a dedicated AI vulnerability database, cataloging failure modes with reproducible evidence. But it leans on community submissions, skews toward bias and broader failure modes, and notes that the definition of an “AI vulnerability” is itself still a working one. Vendor-Specific Disclosures vs. Industry-Wide Registries Disclosure happens vendor by vendor. OpenAI patched the Windows-key jailbreak server-side; Microsoft fixed EchoLeak and issued a CVE. There is no common venue where these land side by side. The Consequences of No Shared Threat Registry for Prompt Injection Fragmented Disclosure Across AI Vendors Each lab discloses on its own terms, on its own blog, if at all. A defender protecting a multi-model stack has to monitor a dozen channels and hope nothing slips by. Duplicate Discovery and Wasted Research Effort Researchers rediscover the same attack repeatedly. The guessing-game jailbreak, the “dead grandma” trick, and other framing attacks are variations on one theme nobody numbered. No Standardized Severity Scoring for
Most security certifications were built for software that follows rules. AI agents do not. They consume data, draw conclusions, call tools, and take action, increasingly without a human in the loop. That gap is what AIUC-1 was created to close: it is the first auditable security standard built specifically for AI agents, and a few enterprise buyers have started asking vendors for it by name. This guide covers what AIUC-1 actually tests, the six risk domains it audits, how the certification process works, what it costs, how long it lasts, and how it aligns with SOC 2, ISO 42001, ISO 27001, and the NIST AI Risk Management Framework. It also covers the structural questions worth asking before you treat an AIUC-1 report as proof of anything. What Is AIUC-1 Certification? AIUC-1 is a certifiable standard for AI agents created by the Artificial Intelligence Underwriting Company (AIUC), a San Francisco-based, venture-backed startup founded by people with experience at organizations including Anthropic. The standard was developed with input from Orrick, Stanford, the Cloud Security Alliance, MIT, and MITRE, and launched in mid-2025. The framework comprises 51 requirements and 130 controls, organized across six risk pillars. It evaluates whether an organization has implemented and tested the technical guardrails, operational practices, and legal policies needed to reduce the risk of unsafe, unreliable, or unauthorized AI behavior. Certification applies to a specific AI system or product, not to the organization as a whole. An AIUC-1 certificate, audit report, and badge tell enterprise buyers that an agent has been independently tested against agent-specific risks. People describe AIUC-1 as the “SOC 2 for AI agents,” and the analogy holds in spirit. The difference is what it looks at. SOC 2 examines a service organization’s general controls. AIUC-1 examines how an agent behaves under pressure: when someone tries to jailbreak it, when it is asked to do something outside its scope, when it has access to data it should not expose. Worth Knowing: About AIUC-1 AIUC-1 does not define what counts as an “AI agent.” The vendor decides which system to certify and what falls in scope. That makes scope the single most important thing to check on any certificate, because a narrowly scoped audit may not cover the agent you actually use. Why AIUC-1 Certification Matters for Enterprise AI Adoption The business case rests on a simple problem: enterprises cannot reliably assess the security of their AI vendors, and the failures are expensive. According to EY research on responsible AI, 64% of companies with over $1 billion in revenue have already lost more than $1 million to AI-related failures. That gap shows up directly in sales cycles. When security, legal, and procurement teams evaluate an AI vendor, they ask about hallucinations, prompt injection defenses, and what happens when an agent makes an unauthorized call. SOC 2 and ISO 27001 do not answer those questions. AIUC-1 gives buyers a structured, third-party-tested answer, which is why holding the certificate can move a stalled procurement review forward. The certification also produces real engineering outcomes, not just a badge. AIUC has reported cases where a customer service agent’s hallucination rate dropped from 11% to under 2% after strengthening its groundedness filter, and another where inappropriate-tone outputs fell from 9% to under 2% through better defensive prompting and output moderation. One company found and patched a PII exposure vulnerability during the certification process itself. The Six Core Risk Domains Covered by AIUC-1 AIUC-1’s 51 requirements are grouped into six domains. Each targets a category of risk that traditional security frameworks were not designed to handle. Data and Privacy Covers how customer data is used, retained, and protected. Requirements address input and output data policies, limits on what data the agent can access, protection of IP and trade secrets, prevention of cross-customer data exposure, and prevention of PII leakage. This is where the standard forces clarity on whether customer data trains the model and how long it is kept. Security The adversarial-resistance domain. It covers third-party testing of adversarial robustness, detection and real-time filtering of malicious inputs, prevention of prompt injection and unauthorized agent actions, enforcement of user access privileges, and protection of the deployment environment. This is the heart of what separates an agent audit from a general security audit. Safety Focuses on preventing harmful and out-of-scope outputs. Requirements include defining an AI risk taxonomy, conducting pre-deployment testing, preventing harmful and customer-defined high-risk outputs, and flagging high-risk outputs for human review. Safety is partly judgment-based, which means documentation alone can sometimes satisfy a requirement, so the testing behind it deserves scrutiny. Reliability Targets the failure modes that erode trust in production: hallucinations and tool misuse. Controls cover hallucination prevention and restrictions on which tools an agent can call and when. For a customer-facing agent, this is the domain that keeps it from inventing a refund policy or triggering the wrong workflow. Accountability Covers what happens when things go wrong. Requirements include AI failure response plans, vendor due diligence, and clear AI disclosure so users know when they are interacting with an agent. With human workers, accountability is built into org charts and chains of command. Agents need an equivalent, and this domain supplies it. Society The broadest domain, focused on preventing misuse with wider consequences: AI-enabled cyber attacks and CBRN (chemical, biological, radiological, nuclear) misuse. Most enterprise agents will touch only a few of these controls, but they matter for higher-capability systems. Insider Note: Of the 130 total controls, roughly 65 are mandatory, and 65 are optional. A straightforward agent typically needs to meet around 40 controls. A complex, multi-modal agent gets closer to 65. The scoping exercise determines which apply, so two AIUC-1 certificates can represent very different amounts of work. Ready to Earn Your AIUC-1 Certification? Accelerate Your AI Certification Journey Talk to an Expert Who Needs AIUC-1 Certification? AIUC-1 is built for any company developing or deploying agentic AI that sells into enterprises. The strongest fit is an organization whose product uses AI agents in customer-facing operations, handles